
Translate this page into:
3T-MRI of finger pulleys - Review of anatomy and traumatic conditions involving them

First author: Sanjay Desai, Department of Radiodiagnosis, Deenanath Mangeshkar Hospital, Pune, Maharashtra, India. drsanjaydesai@gmail.com
*Corresponding author: Amith Gaitonde, Department of Radiodiagnosis, Deenanath Mangeshkar Hospital, Pune, Maharashtra, India. amitgaitonde03@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Desai S, Gaitonde A, Subramanian S, Lokhande P, Asthana K. 3T-MRI of finger pulleys - Review of anatomy and traumatic conditions involving them. Indian J Musculoskelet Radiol. 2023;5:77-81. doi: 10.25259/IJMSR_22_2023
Abstract
Injuries to the pulleys often occur in overuse injuries (climbers) and in traffic accidents involving the fingers. The anatomy of the pulleys of the thumb is different from that of the other four fingers. With 3 Tesla magnetic resonance imaging injuries to the pulleys can be diagnosed by direct and indirect signs. We should be familiar with the anatomy and injuries of the finger pulleys so that we can make an accurate diagnosis, determine the extent, and degree of the pulley injuries, and treat the patient accordingly.
Keywords
Finger pulleys
Pulley injury
Rock climbers
Bowstring
pulleys

INTRODUCTION
Injuries to the finger pulleys often occur due to overuse, particularly in climbers, or as a result of traffic accidents. These pulley injuries lead to painful movement and weaker grip. The lower-grade pulley injuries are managed conservatively and higher-grade injuries need surgical intervention. Magnetic resonance imaging (MRI) helps in accurate diagnosis, determining the extent, and degree of the pulley injuries. Based on this, the appropriate decisions for patient management can be taken.
PROTOCOL
The patient is positioned in a supine position with the arms by the side in a hand/wrist receiver-only coil, if available. The imaging protocol included a proton density fat-saturated sequence (PDFS) of the hand in the coronal plane. It is followed by dedicated imaging of the injured finger and adjacent unaffected finger in axial, coronal, and sagittal planes. The sequences acquired at our institution are described in Table 1.[1]
| T1 sagittal |
| PDFS sagittal |
| PDFS transverse |
| T1 transverse |
| PDFS coronal |
| PDFS sagittal sequence when the finger flexed as much as possible (if pulley injury is suspected) |
MRI: Magnetic resonance imaging, PDFS: Proton density fat-saturated sequence
ANATOMY AND FUNCTION OF FINGER PULLEY (2ND–5TH FINGERS)
The anatomy of the pulleys of the thumb and the rest of the fingers are slightly different.
The flexor digitorum profundus and superficialis tendons of the second through fifth fingers glide within the synovium-lined fibrous sheaths when the muscle contracts. The pulleys are localized thickenings of the fibrous sheath. They ensure that the flexor tendons and adjacent phalanges remain in close alignment during flexion.[2] As a result, more finger flexion can be achieved with every contraction of the muscles.[3]
There are five annular Figure 1 and three cruciate pulleys. The first, third, and fifth annular pulleys, that is, A1, A3, and A5 pulleys, are at the levels of metacarpophalangeal (MCP), proximal interphalangeal (PIP), and distal interphalangeal (DIP) joints, respectively. The second annular pulley (A2) is at the level of the proximal and mid-diaphysis of the proximal phalanx. The fourth annular pulley (A4) attaches to the middiaphysis of the middle phalanx [Table 2].
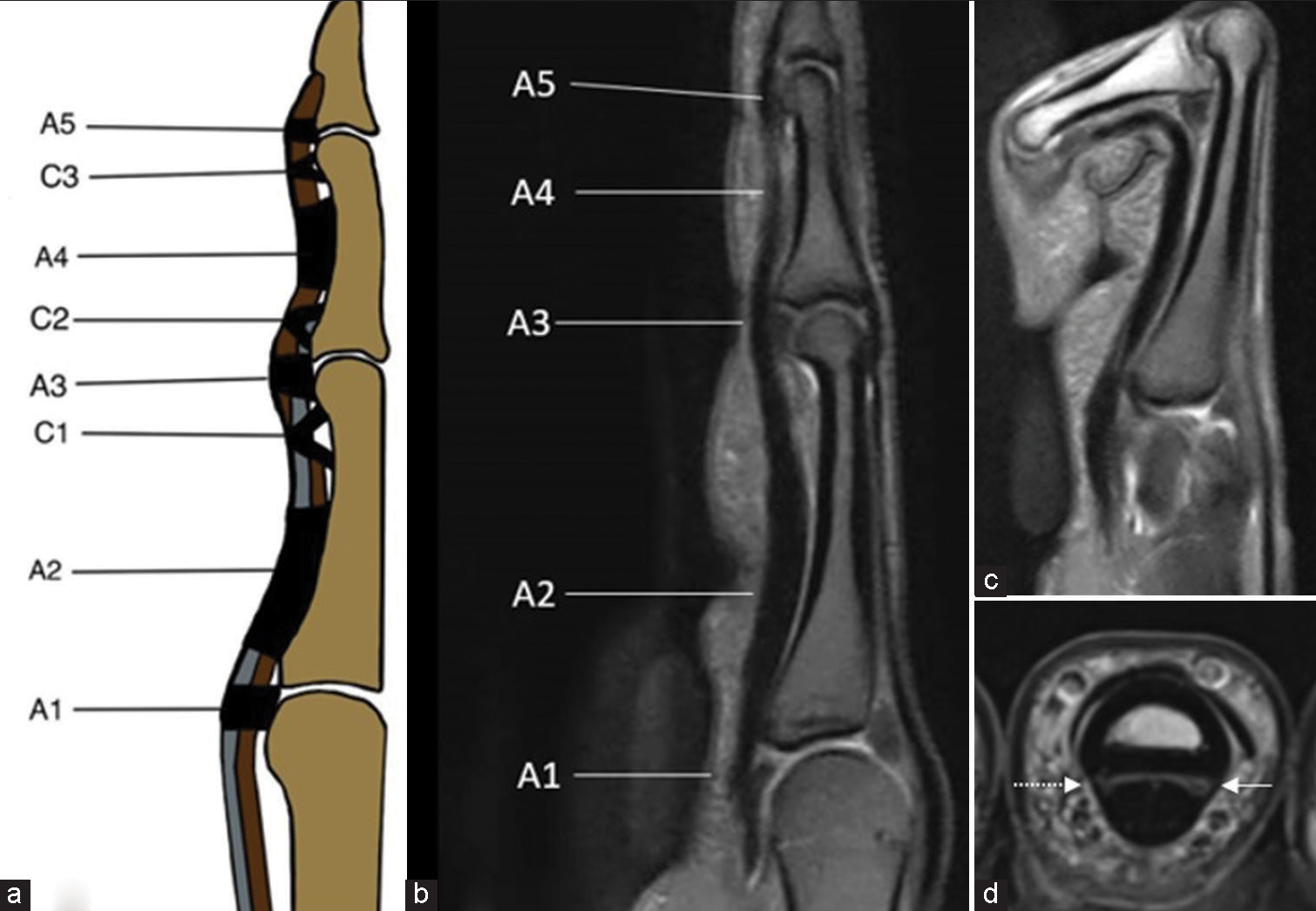
- (a) Sagittal anatomical image, (b) proton density fat-saturated sequence (PDFS) sagittal neutral, (c) PDFS flexed position, (d) T1 axial images. (a) shows A1–A5 annular pulleys and C1–C3 pulleys. T1 axial image (d) shows the ulnar limb (white solid arrow) and radial limb (dotted arrow) of the pulley
| Pulleys of 2nd–5th fingers | Levels and attachments of the pulleys |
|---|---|
| A1 | Metacarpophalangeal Joint (Volar plate and head of the metacarpal) |
| A2 | Proximal and mid-diaphysis of the proximal phalanx |
| C1 | Between the A2 and A3 pulleys |
| A3 | Proximal interphalangeal joint (Volar plate and head of the proximal phalanx) |
| C2 | Between A3 and A4 pulleys |
| A4 | Mid-diaphysis of the middle phalanx |
| C3 | Between A4 and A5 pulleys |
| A5 | Distal interphalangeal joint (Volar plate and head of the middle phalanx) |
The pulleys at the level of the joints insert onto the volar plates and pulleys at the level diaphysis of phalanges insert into the volar aspect of the bone.[4] The pulleys at the level of the joints, that is, A1, A3, and A5 pulleys, are inserted on the volar plate and respective proximal bone. Two-thirds of the pulley is inserted into the volar plate and one-third is inserted into the proximal bone. For example, two-thirds of the A1 pulley inserts onto the volar plate and one-third of the pulley inserts into the head of the metacarpal.
The cruciate pulleys are also thickenings of the finger fibrous sheaths and are attached to the underlying bone at these levels [Table 1]. There are three cruciate pulleys in the finger: C1, C2, and C3. The first one is placed between A2 and A3, the second one between A3 and A4, and the third one between A4 and A5.
At present 3 Tesla (3T)-MRI resolution, the annular pulleys are well-visualized under optimum technical conditions, although better visualized in the presence of fluid within tendon sheaths. The cruciate pulleys are not optimally visualized in a 3T-MRI scanner. The most important pulleys to prevent bowstringing are the A2, A3, and A4 annular pulleys.[5]
MRI ANATOMY OF THUMB
In contrast to the pulleys of other fingers, there are three annular and one oblique pulley in the thumb. The annular pulleys are transverse to the long axis of the thumb [Figure 2].
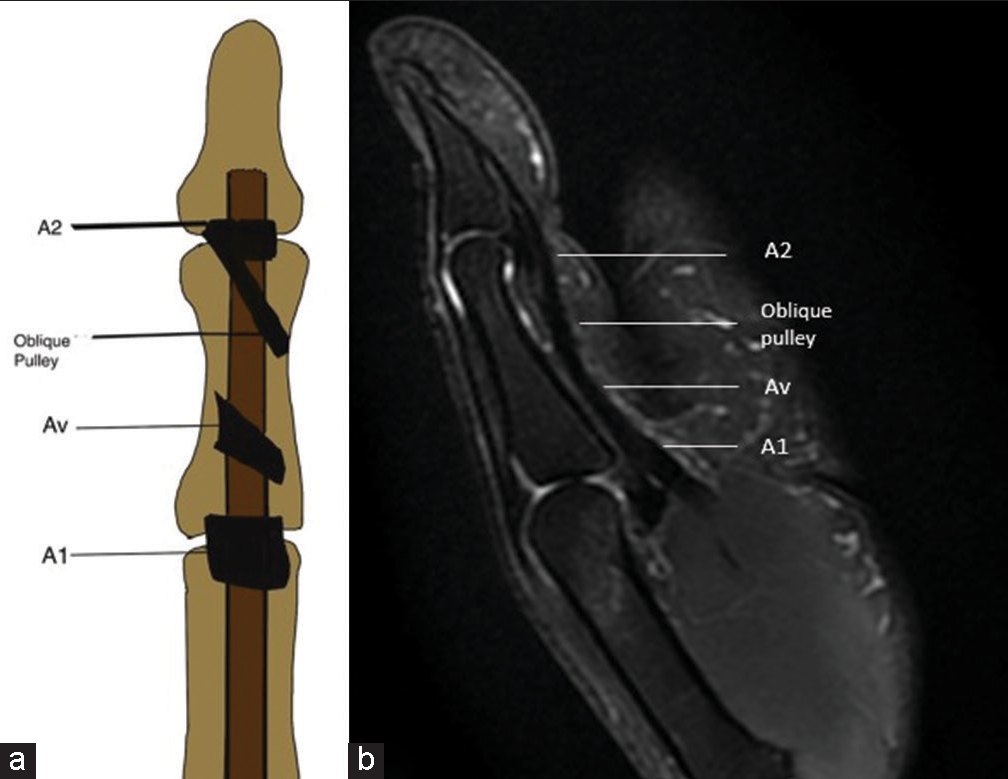
- (a) Coronal anatomical image, (b) Proton density fat-saturated sequence sagittal image of the thumb showing A1, Av, oblique and A2 pulleys.
The first annular pulley (A1) is at the level of the MCP joint. The majority of this pulley inserts into the volar plate and fibers also attach to the base of proximal phalanx.[6]
The variable annular pulley (AV) is located at the base of the proximal phalanx. It can have either a transverse or oblique orientation.[7]
The oblique pulley (A oblique) originates from the ulnar aspect of the proximal shaft of the proximal phalanx and inserts into the radial aspect of the base of the distal phalanx. The AV and oblique pulleys are continuous with adductor pollicis tendons sheath.
The (A2) annular pulley is at the level of the base of the distal phalanx. The majority of this pulley inserts into the base of the distal phalanx with few fibers insertion into the volar plate.
The oblique and A1 annular pulleys are important in maintaining the flexor pollicis tendon in place and preventing bowstringing. The A2 pulley is the least important among the thumb pulleys to maintain the function.[8]
On MRI imaging, the finger pulleys can be visualized on PDFS sagittal and axial images. They appear as hypointense bands along the volar fibrous sheaths of the finger at various locations described above. Initially, the pulleys are localized on sagittal images and then they are correlated in axial images to check for integrity.
INJURIES OF THE FINGER PULLEYS
Injuries of finger pulleys are most common in rock climbers. In these people, there is flexion at the MCP and PIP joints due to the action of flexor tendons and extension at the DIP joint which causes extensive stress on the pulleys and results in tears.[9] However, it is not exclusive to them, they can occur in many other traumatic conditions (vehicular accidents). The most commonly injured pulley is the A2 pulley, followed by the A3 and A4 pulleys.[10] There can be isolated pulley injuries or associated with other injuries of the fingers.
Clinically, the patient presents with swelling and pain and sometimes gives a history of hearing popping sounds. Damage to pulleys decreases the torque at the DIP and PIP joints during flexion and extension of fingers. The patient is unable to flex the finger fully.[11]
MRI helps in the early diagnosis and grading of pulley injuries which helps in patient management. The less severe injuries are managed conservatively; however, higher-grade injuries require surgical management. There are three grades of pulley injuries. The grade 1 injury is a sprain in the pulley. It is seen as edema within and adjacent to the pulley with no disruption of fibers. Usually, MRI is not done for isolated grade 1 injuries of the pulley. In the grade 2 injury, there is a partial tear of the pulley. On MRI there is partial discontinuity of the pulley with edema (fluid) superficial and deep to the pulley [Figure 3]. However, there is no significant increase in the distance between the tendon and the underlying bone.[12] In grade 3 pulley injury, there is a complete rupture of the pulley. On MRI, there is non-visualization of the pulley with fluid intensity at the site of the injury [Figures 4 and 5]. This is a direct sign of pulley injury. However, sometimes it may be difficult to visualize the finger pulley even in uninjured patients. Relying completely on direct visualization of the torn pulleys on axial images may lead to overdiagnosis of pulley injury. Hence, one should also look for indirect signs of pulley injury which are increased gaps between the flexor tendon and underlying bone on both sagittal and axial images.[13] In case of suspected pulley injury, another PDFS sagittal image is acquired in a flexed position. In this position, there is an increase in the gap as compared to the neutral position which is referred to as the “bowstring sign”[14] [Figures 6 and 7]. The longitudinal extent and degree of the bowstringing of the tendon from bone depend on the number of pulleys injured. A comparison is done of this gap with the adjacent uninjured finger on axial images.
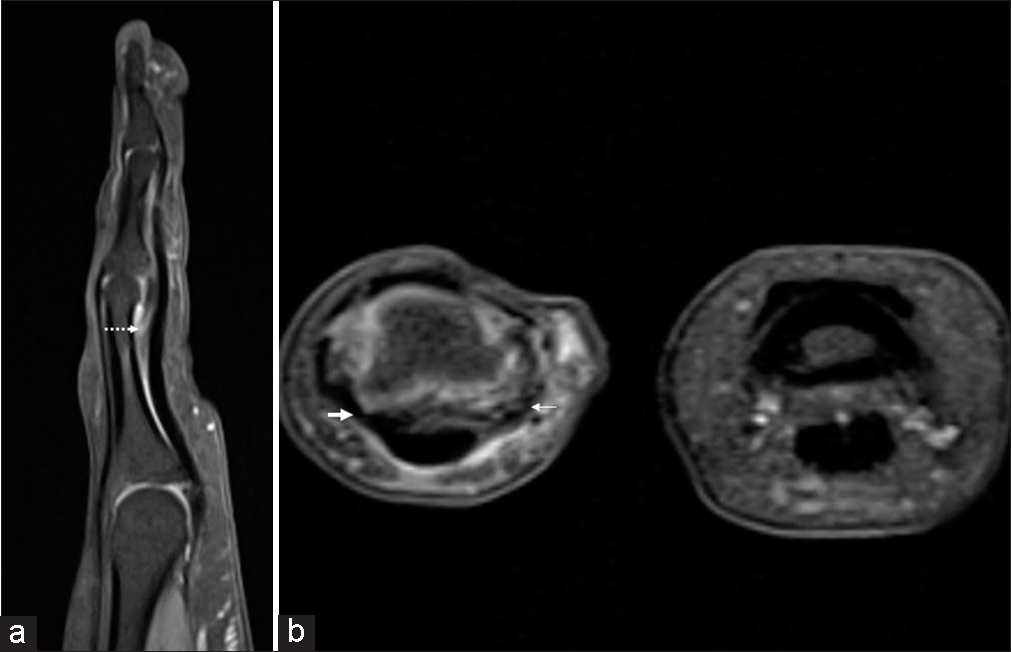
- (a) Proton density fat-saturated sequence (PDFS) sagittal and (b) PDFS axial images, show partial tear of limbs radial (thin arrow) the A3 annular pulley. The ulnar limb (thick arrow) is intact. There is minimal fluid collection distance (dotted arrow) deep to the flexor tendon and volar plate with no increased distance between the tendon and phalanx-Schoff grade II (Grading explained later).
- (a) Proton density fat-saturated sequence sagittal and (b) axial images, show complete tear of ulnar (thick arrow) and radial (thin arrow) limbs the A2 annular pulley. There is fluid collection and increased distance (dotted arrow) between the flexor tendons and proximal phalanx is also noted indicating A2 pulley rupture (indirect sign)- Schoff grade III.
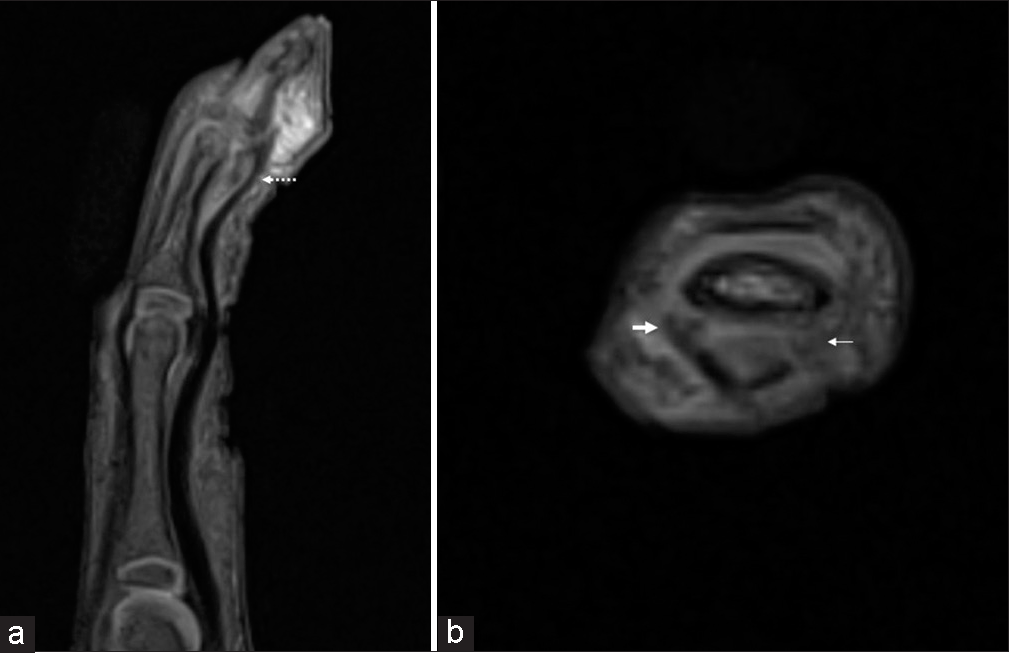
- (a) Proton density fat-saturated sequence sagittal and (b) axial images, show near complete tear of radial limb (thick arrow) and complete tear of the ulnar limb (thin arrow) the A5 annular pulley. There is fluid collection and increased distance (dotted arrow) between the flexor tendons and proximal phalanx is also noted indicating A5 pulley rupture (indirect sign) - Schoff grade II.
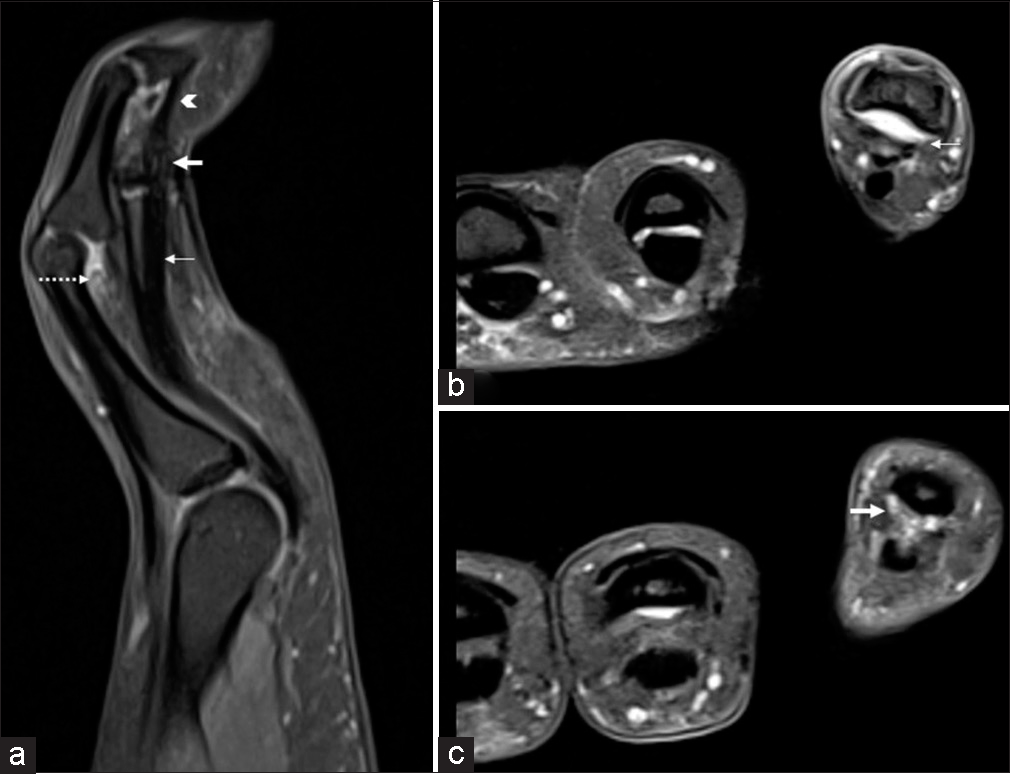
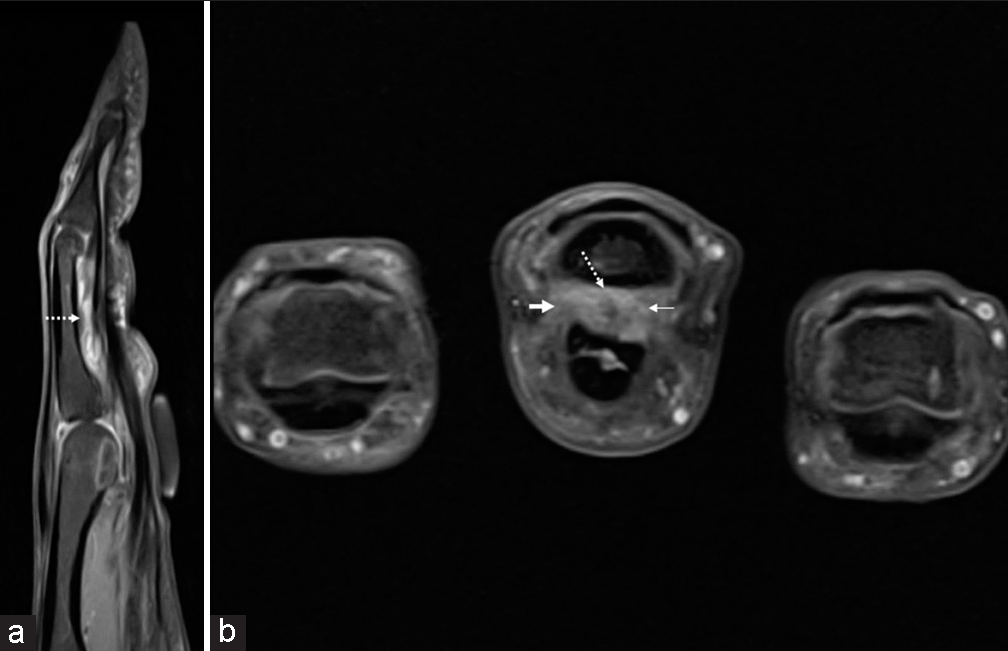
- (a) Proton density fat-saturated sequence sagittal, (b, c) axial images, show complete tears of A3 (thin arrow), A4 (thick arrow) and A5 (arrow head) pulleys. There is fluid collection and increased distance (dotted arrow) between the flexor tendons and proximal phalanx (indirect sign) -Schoff grade IV.
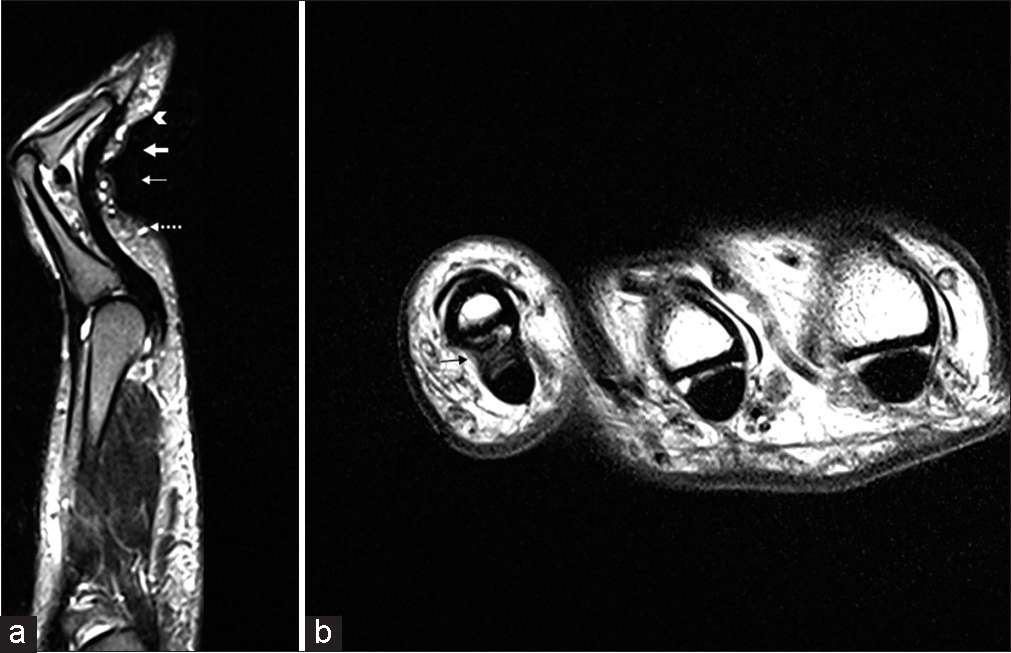
- (a) Proton density (PD) sagittal, (b) PD axial images, show complete tears of A2 (dotted arrow), A3 (thin white arrows), and A4 (thick arrow) with intact A5 (arrow head) pulleys. There is fluid collection and increased distance between the flexor tendons and proximal phalanx (indirect sign) - Schoff grade IV.
Schöffl et al. graded pulley injuries as follows:[15]
Grade 1: Sprain of the pulley
Grade 2: Partial tear of A2/A3 pulleys or complete tear of A4 pulley
Grade 3: Complete tear of A2/A3 pulleys
Grade 4: Multiple pulley tear or single pulley tear associated with injuries lumbricals or collateral ligaments
Grade 1–3 injuries require conservative management and grade 4 injuries require surgical intervention.
CONCLUSION
Pulley tears are common in overuse injuries (rock climbers) as well as vehicular accidents involving the fingers. 3T-MRI can be used for accurate diagnosis, to establish the extent, and to grade the pulley injuries for appropriate patient management.
Ethical approval
The research/study complied with the Helsinki Declaration of 1964.
Declaration of patient consent
Patient’s consent is not required as the patient’s identity is not disclosed or compromised.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The author(s) confirms that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- MRI sport-specific pulley imaging. Skeletal Radiol. 2018;47:989-92.
- [CrossRef] [PubMed] [Google Scholar]
- Magnetic resonance imaging in orthopedic sports medicine Berlin: Springer Science and Business Media; 2008.
- [CrossRef] [Google Scholar]
- Kinesiology of the musculoskeletal system: Foundation for rehabilitation. Vol 350. (3rd ed). St. Louis, MO: Mosby Elsevier; 2017. p. :368.
- [Google Scholar]
- Pulley system in the fingers: Normal anatomy and simulated lesions in cadavers at MR imaging, CT, and US with and without contrast material distention of the tendon sheath. Radiology. 2000;217:201-12.
- [CrossRef] [PubMed] [Google Scholar]
- Injury to the A2 pulley in rock climbers. J Hand Surg Br. 1990;15:268-70.
- [CrossRef] [PubMed] [Google Scholar]
- Anatomy of the finger flexor tendon sheath and pulley system. J Hand Surg Am. 1988;13:473-84.
- [CrossRef] [PubMed] [Google Scholar]
- The pulley system of the thumb: Anatomic and biomechanical study. J Hand Surg Am. 2002;27:628-35.
- [CrossRef] [PubMed] [Google Scholar]
- Biomechanics of the thumb flexor pulley system. J Hand Surg Am. 1994;19:475-9.
- [CrossRef] [PubMed] [Google Scholar]
- Overuse injuries in the elite rock climber. Med Sci Sports Exerc. 2000;32:1369-72.
- [CrossRef] [PubMed] [Google Scholar]
- Pathomechanics of closed rupture of the flexor tendon pulleys in rock climbers. J Bone Joint Surg Am. 1998;80:1012-9.
- [CrossRef] [PubMed] [Google Scholar]
- A potentially inexpensive diagnostic method for A2 pulley ruptures. Cureus. 2019;11:e5751.
- [CrossRef] [PubMed] [Google Scholar]
- The athlete's hand: Ligament and tendon injury. Semin Musculoskelet Radiol. 2010;16:338-50.
- [CrossRef] [PubMed] [Google Scholar]
- Disruption of the finger flexor pulley system in elite rock climbers. Am J Sports Med. 1998;26:651-5.
- [CrossRef] [PubMed] [Google Scholar]
- Bowstring injury of the flexor tendon pulley system: MR imaging. AJR Am J Roentgenol. 1996;167:347-9.
- [CrossRef] [PubMed] [Google Scholar]
- Pulley injuries in rock climbers. Wilderness Environ Med. 2003;14:94-100.
- [CrossRef] [PubMed] [Google Scholar]




