
Translate this page into:
A rare case report of proximal focal femoral deficiency associated with fibular hemimelia

*Corresponding author: Riya Samanta, Department of Radiology, Mahajan Imaging and Labs, Safdurjung Hospital, Sports Injury Centre, New Delhi, India. samanta.ria1011@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Samanta R, Batta NS. A rare case report of proximal focal femoral deficiency associated with fibular hemimelia. Indian J Musculoskelet Radiol. 2025;7:134-6. doi: 10.25259/IJMSR_68_2024
Abstract
Proximal focal femoral deficiency (PFFD) is a rare congenital condition characterized by the partial or complete absence of the proximal femur, which can affect the hip joint and leg length. The severity of PFFD varies widely; some individuals may have significant limb shortening and malformation, while others may have a more functional limb. It is associated with various other osseous abnormalities, among which ipsilateral fibular agenesis or hemimelia is most frequently seen. We present an interesting case of a 28-year-old male with PFFD presenting with limb length discrepancy and describe the clinicoradiological features and associated abnormalities in this case. Our patient had hypoplastic left hemipelvis, markedly shallow and dysplastic left acetabulum, very small left femoral head which was not articulated with the femoral shaft and was displaced in a posterosuperior direction. In addition, a shortened femoral segment was noted, with the distal femoral condyle visible and a tapered proximal end. Absent left patella, fibular hemimelia with undeveloped proximal portion, heel valgus, and midfoot varus were also noted.
Keywords
Acetabular dysplasia
Aitken classification
Congenital short femur
Fibular hemimelia
Proximal focal femoral deficiency

INTRODUCTION
Proximal focal femoral deficiency (PFFD), also known as proximal femoral dysgenesis[1] and congenital short femur,[2] is a rare congenital anomaly characterized by the absence of one-third to two-thirds of the proximal femur.[3] The incidence of PFFD is reported to be between 1.1 and 2.0/100,000 live births.[4] The precise etiology of this disorder remains unclear; however, it has been associated with a defect in the primary ossification center of the cartilage anlage.[5] PFFD is often linked to various osseous anomalies, including fibular hemimelia, absent patella, and acetabular dysplasia, with ipsilateral fibular hemimelia being the most frequently observed association. Notably, some portion of the femur is invariably present in affected individuals, differentiating this condition from phocomelia and complete femoral agenesis.[6] The implications of this anomaly include impaired growth, limb length discrepancy, and gait abnormalities. Among the several classification systems proposed, Aitken’s classification[7] is the most widely utilized, categorizing PFFD into four classes based on the anatomical relationship between the acetabulum and the proximal femur [Table 1].
| Class A (least severe) | Femoral head is present and attached to the shaft by femoral neck A cartilaginous neck may not be seen in early radiograph which ossifies later Sometimes, the cartilaginous connection between the neck and shaft may form a subtrochanteric pseudoarthrosis Short femur and coxa vara present. |
| Class B | Acetabulum may be adequate or moderately dysplastic The femoral head is contained in the acetabulum No osseous connection present between the femoral head and shaft at maturity Short femoral segment with a bulbous bony tuft. |
| Class C | Severe acetabular dysplasia Absent or very small femoral head, not attached to the shaft Short femoral segment with a tapered proximal end. |
| Class D (most severe) | Absent acetabulum and proximal femur No proximal tuft present. |
PFFD: Proximal femoral focal deficiency
CASE REPORT
A 28-year-old male with a history of left lower-limb shortening by birth presented with complaints of pain in the left hip and knee joints for a duration of 2 months. The patient reported no significant antenatal or family history, and there was no history of trauma. Clinical examination revealed a shortened left lower limb with notable limb length discrepancy and soft-tissue atrophy. Range of motion in the left hip was significantly limited, while flexion of the left knee joint was unaffected. Assessment of the left ankle joint indicated restricted dorsiflexion. The examination of the right lower limb and both upper limbs was unremarkable. Radiological assessment identified significant abnormalities in the left proximal femur. The left hemipelvis was hypoplastic, and the left acetabulum was markedly shallow and dysplastic. A very small left femoral head was observed, which was not articulated with the femoral shaft and was displaced in a posterosuperior direction. In addition, a shortened femoral segment was noted, with the distal femoral condyle visible and a tapered proximal end. The tibiofemoral joint space was preserved, and left patella was absent [Figure 1].
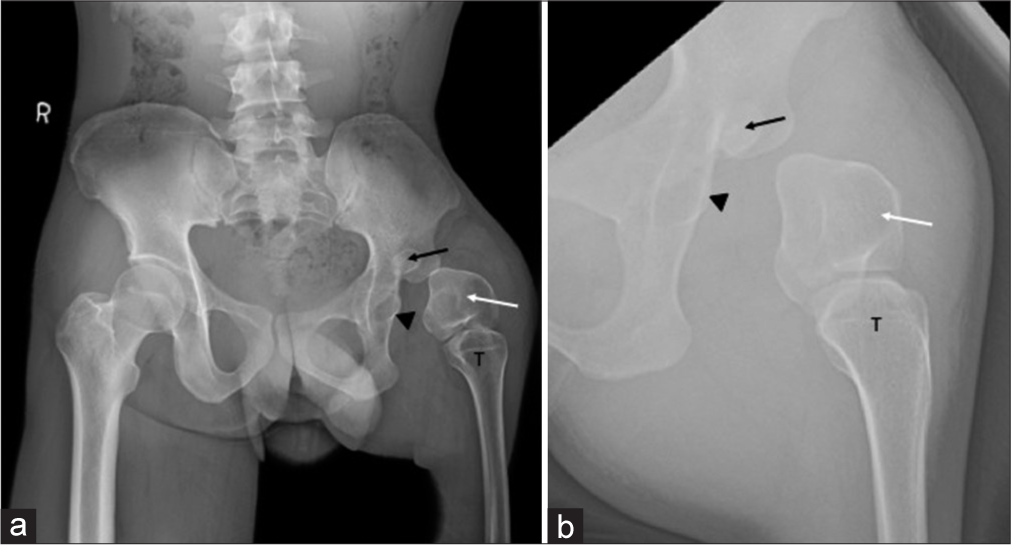
- (a and b) Proximal focal femoral deficiency-Aitken Class C. (a) Digital X-ray of the pelvis with both hip joints and (b) the left hip (zoomed) anteroposterior view reveals hypoplastic left hemipelvis, markedly shallow and dysplastic left acetabulum (arrowheads), very small left femoral head (black arrows), not attached to the shaft and displaced posterosuperiorly, short femoral segment (distal femoral condyle seen) with a tapered proximal end (white arrows), preserved tibiofemoral joint and absent left patella. The left proximal tibia has been marked (T).
Radiographs of the left lower limb and left foot revealed normal left tibia, fibular hemimelia with undeveloped proximal portion, heel valgus, and midfoot varus [Figure 2]. A diagnosis of PFFD, classified as Aitken type C, was established.

- (a-c) Digital X-ray of the (a) left lower limb, (b) oblique and (c) anteroposterior view of the left foot show left proximal focal femoral deficiency-Aitken Class C (white arrow in a), normal left tibia (T in a), fibular hemimelia with undeveloped proximal portion (black arrow in b and c), heel valgus (asterisk in b), and midfoot varus (dashed arrows in b).
Since this patient with PFFD presented in late adulthood, at which point significant bone loss has occurred, rendering surgical intervention no longer feasible. Given these circumstances, the most appropriate therapeutic approach is the use of prosthetics, which can help maintain a high quality of life by enabling the patient to remain independent and mobile. A diagnosis of suggesting PFFD-Aitken class C was made and the patient was referred to the orthopedic clinic with radiographs for management.
DISCUSSION
PFFD is a rare congenital osseous abnormality of the development of proximal femur, the patho-anatomy of which remains obscure and is often linked to the abnormal development of the common cartilage anlage of the ilium and proximal femur.[6] Heredity does not appear to play a major role in its development. Disturbances at cellular level secondary to infection, nutritional disorder, or vascular insults have been postulated as possible causes. It may be associated with a number of other osseous abnormalities such as fibular hemimelia, absent patella, and acetabular dysplasia.[6] It results in impaired growth, limb length discrepancy, and gait abnormalities. Based on the severity of the abnormality, Aitken classification has been postulated with class A being the least severe and class D being the most severe form.[7] Radiographic evaluation plays a vital role in classifying and assessing the severity of PFFD, the associated osseous abnormalities, and enabling appropriate management.
Management of PFFD necessitates a multidisciplinary approach, incorporating pediatric orthopedic surgeons, prosthetists, and physiotherapists to optimize function and mobility. Treatment strategies should be tailored based on the degree of femoral shortening, musculature status, and the integrity of hip and knee joints, as well as leg and foot deformities.[8,9] Early identification through clinical and radiological assessment is essential for timely intervention, which can significantly enhance walking ability and overall quality of life, thereby promoting optimal limb growth and development.
CONCLUSION
PFFD, also known as proximal femoral dysgenesis or congenital short femur, is a rare osseous anomaly that may present in isolation or in conjunction with other skeletal abnormalities. This condition leads to limb length discrepancy and gait abnormalities. Radiographic evaluation is essential for classifying PFFD and assessing its severity. Timely clinical and radiological assessment is critical for facilitating appropriate interventions, ultimately promoting improved limb growth and development.
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship: Nil.
References
- Dysgenesis of the proximal femur (coxa vara) and its surgical management. J Bone Joint Surg. 1962;44A:1-24.
- [CrossRef] [Google Scholar]
- Congenital short femur. Simple femoral hypoplasia. J Bone Joint Surg. 1959;418:73-9.
- [CrossRef] [PubMed] [Google Scholar]
- Proximal femoral focal deficiency. Am J Roentgenol. 1978;131:289-95.
- [CrossRef] [PubMed] [Google Scholar]
- Proximal femoral focal deficiency-a rare congenital entity: Two case reports and a review of the literature. J Med Case Rep. 2020;14:1-6.
- [CrossRef] [PubMed] [Google Scholar]
- Proximal femoral focal deficiency (PFFD) imaging spectrum. J Med Sci Res. 2015;3:90-3.
- [CrossRef] [Google Scholar]
- Proximal femoral focal deficiency (PFFD) Radiology. 1977;125:197-203.
- [CrossRef] [PubMed] [Google Scholar]
- Proximal femoral focal deficiency: Definition, classification, and management In: Paper presented at a Symposium on Proximal Femoral Focal Deficiency, Washington, DC, 1968. Washington, DC: National Academy of Sciences; 1969.
- [Google Scholar]
- Principles of rotationplasty. J Am Acad Orthop Surg. 2012;20:657-67.
- [CrossRef] [PubMed] [Google Scholar]
- Unilateral short femur-what does this mean? Report of 3 cases. Ultrasound Q. 2008;24:89-92.
- [CrossRef] [PubMed] [Google Scholar]




