
Translate this page into:
Atypical case of wrist pain in young with Madelung deformity
 , Bhamidipaty Kanaka Durgaprasad1, Naga Varaprasad Vemuri2
, Bhamidipaty Kanaka Durgaprasad1, Naga Varaprasad Vemuri2

*Corresponding author: Vineet Kumar Vemuri, Department of Radiodiagnosis, GITAM Institute of Medical Sciences and Research, Visakhapatanam, Andhra Pradesh, India. vineetradiology97@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Vemuri VK, Madhu Mallik GR, Durgaprasad BK, Vemuri NV. Atypical case of wrist pain in young with Madelung deformity. Indian J Musculoskelet Radiol. 2024;6:125-7. doi: 10.25259/IJMSR_50_2024
Abstract
The Vickers ligament is a distinct ligamentous structure that connects the lunate bone and the triangular fibrocartilage complex to the distal radius. It is commonly present in individuals with Madelung deformity, a congenital malformation of the wrist. This ligament restricts the normal growth and movement of the radius, contributing to the characteristic wrist deformity and often leading to pain and functional limitations. Madelung deformity is frequently observed in young females and often presents with symptoms of wrist pain, restricted range of motion, and visible deformity. Here, we describe an intriguing case of a young female patient who presented with wrist pain and was found to have Madelung deformity in her left wrist. This case highlights the importance of recognizing Vickers ligament as a contributing factor to the patient’s symptoms and the deformity’s progression.
Keywords
Vickers ligament
Madelung deformity
Magnetic resonance imaging

INTRODUCTION
Madelung deformity is a congenital wrist condition, frequently linked to mutations in the SHOX gene, and can often manifest bilaterally.[1] A key feature of this deformity is the presence of the Vickers ligament, also known as the radiolunate ligament, which is a short, thick ligament originating from the volar aspect of the distal radius and inserting into the lunate bone, commonly found in individuals with Madelung deformity.[2] In addition, the anomalous volar radiotriquetral ligament is another ligament associated with this condition.[3]
The Vickers ligament extends across the ulnar aspect of the distal radius, contributing to the distinctive volar and ulnar angulation observed in Madelung deformity. These ligaments play a central role in the pathophysiology of the deformity by creating a tethering effect that restricts growth and alters normal wrist development, exacerbating the abnormal growth patterns of the distal radius. The main clinical concerns for individuals with Madelung deformity include wrist pain, functional impairment, and visible deformity.[1-3]
Here, we describe an intriguing case of a young female patient who presented with wrist pain and was found to have Madelung deformity in her left wrist. This case highlights the importance of recognizing Vickers ligament as a contributing factor to the patient’s symptoms and the deformity’s progression.
CASE REPORT
A 12-year-old female presented with left wrist pain, with no reported history of trauma. Frontal and lateral radiographs of the left wrist revealed mild dorsal bowing and pronounced radial bowing of the distal radius, accompanied by dorsal subluxation of the ulnar head and a positive ulnar variance [Figures 1a and 1b]. The radiographs also showed a medial and downward inclination of the distal radial metaphysis, with shortening and hypoplasia of the radial physis on the ulnar side. In addition, there was an increased lunate fossa angle, wedging of the proximal carpal row, and proximal migration of the lunate with evidence of lunate subsidence [Figure 1a].

- (a) Frontal and (b) lateral radiographs of the left hand demonstrate Madelung deformity with positive ulnar variance. There is lunate subsidence and wedge-shaped proximal carpal row. Dorsal subluxation of the ulnar head is causing “bayonet” like deformity.
An magnetic resonance imaging (MRI) of the left wrist was performed using T1-weighted images in axial and coronal planes; T2-weighted imaging in coronal, axial, and sagittal planes; proton density fat-saturated images in coronal and sagittal planes; and short tau inversion recovery in coronal sections. A minimal amount of free fluid was observed in the left distal radioulnar joint space. In addition, a thick, band-like ligament was identified at the volar aspect of the distal radius, originating from the metaphysis proximal to the radial epiphysis and inserting on the ulnar margin of both the lunate and triquetral bones, representing the radiolunate and radiotriquetral ligaments [Figure 2a-d].
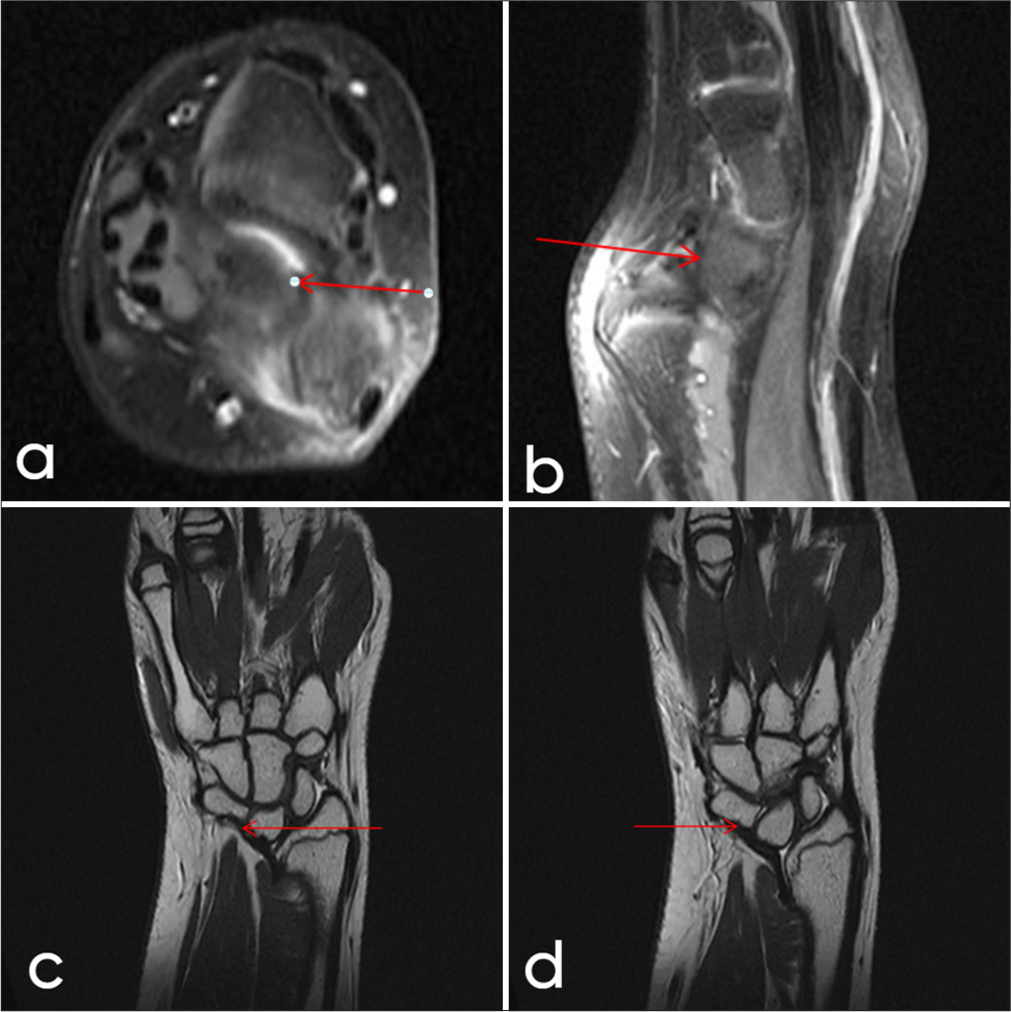
- A 12-year-old female. (a) Axial T2, (b) sagittal, (c) coronal fluid sensitive magnetic resonance sequences showing radiolunate (Vickers ligament) (red arrow) with associated madelung deformity. (d) Coronal T2W image showing radiotriquetral ligament (red arrow).
Further findings included T2/PD hyperintensities in the ulnar head, suggestive of bone marrow edema, as well as hyperintensity around the extensor carpi ulnaris tendon, consistent with tendinosis. Thinning of the radial epiphysis on the ulnar side and mild proximal migration of the lunate were also noted.
DISCUSSION
The Vickers ligament is an anomalous structure frequently associated with Madelung deformity, a congenital wrist disorder marked by abnormal growth and curvature of the radius, often causing wrist pain and limited range of motion. Named after Dr. Vickers, who initially described it, this ligament arises from the volar aspect of the distal radius and attaches to the lunate bone, restricting the normal growth and mobility of the wrist.[1-3]
In Madelung deformity, the Vickers ligament (or radiolunate ligament) connects the lunate bone and the triangular fibrocartilage complex to the distal radius and is present in the majority of affected patients. The condition commonly affects children aged 8–14, with a higher prevalence in females (female-to-male ratio of 4:1). Madelung deformity is also associated with several genetic and syndromic conditions, such as Turner syndrome, nail-patella syndrome, gonadal dysgenesis, and diaphyseal aclasis.[4]
A radial notch at the attachment site of the Vickers ligament and the presence of this anomalous radiolunate ligament can help differentiate Madelung-type deformities from true congenital Madelung deformities.[5] Various conditions can produce a Madelung-like or pseudo-Madelung deformity; however, they lack the characteristic Vickers ligament or the anomalous radiotriquetral ligaments seen in true Madelung deformity [Table 1]. MRI is the preferred imaging modality for visualizing the Vickers ligament and related abnormalities associated with Madelung deformity. This imaging allows for optimal assessment of the commonly associated radiolunate ligament and, less frequently, the radiotriquetral ligament.
| S. No. | Differential diagnosis | Differentiating features |
|---|---|---|
| 1. | Pseudo-Madelung Deformity | Characterized by negative ulnar variance, resulting in radial deviation |
| 2. | Multiple Epiphyseal Dysplasia and Ollier Disease | Morphologically similar to classic Madelung deformity, but lacks the presence of the Vickers ligament or anomalous radiotriquetral ligament |
| 3. | Turner’s syndrome | May show decreased carpal angles resembling Madelung deformity but is also associated with a shortened 4th metacarpal and osteopenia |
| 4. | Infection or Chronic Arthritis | Infection or inflammation can lead to premature closure of the epiphysis, resulting in a pseudo-Madelung-like deformity |
In addition, MRI can identify other pathologies such as tendinitis and joint effusions. In some cases, radiolunate dislocation due to the Vickers ligament may be visible on both forearm radiographs and MRI.[3]
Madelung deformity may present as an isolated condition or with symptoms such as discomfort, wrist pain, reduced grip strength, and limited wrist mobility.[6] For individuals with mild symptoms, conservative treatment with non-steroidal anti-inflammatory drugs (NSAIDs) and activity modification may be effective.[7] In young patients with progressive deformity, surgical resection of the Vickers ligament and any anomalous radiotriquetral ligament can alleviate symptoms and help prevent further progression. For those who have reached skeletal maturity and experience persistent pain or restricted wrist mobility, surgical intervention may be considered to improve function.[8,9]
CONCLUSION
Madelung deformity is a rare congenital condition often associated with the anomalous Vickers ligament, which restricts normal wrist development and contributes to pain, deformity, and limited wrist function. This case emphasizes the role of MRI in identifying the Vickers ligament and associated anomalies, which are pivotal in distinguishing true Madelung deformity from similar conditions and pseudo-Madelung deformities. In managing symptomatic cases, conservative approaches such as NSAIDs and activity modifications are effective for mild symptoms, while surgical intervention may be required in progressive or severe cases to improve wrist function and alleviate pain. Early recognition and appropriate treatment of Madelung deformity are crucial in mitigating long-term morbidity and functional impairment.
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript, and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Radiological and clinical analysis of Madelung's deformity in children. Orthop Traumatol Surg Res. 2014;100:S349-52.
- [CrossRef] [PubMed] [Google Scholar]
- Madelung deformity: Surgical prophylaxis (physiolysis) during the late growth period by resection of the dyschondrosteosis lesion. J Hand Surg Br. 1992;17:401-7.
- [CrossRef] [PubMed] [Google Scholar]
- MRI appearance of the anomalous volar radiotriquetral ligament in true Madelung deformity. Skeletal Radiol. 2019;48:915-8.
- [CrossRef] [PubMed] [Google Scholar]
- Distal radioulnar joint: Normal anatomy, imaging of common disorders, and injury classification. Radiographics. 2023;43:e220109.
- [CrossRef] [PubMed] [Google Scholar]
- Madelung deformity and Madelung-type deformities: A review of the clinical and radiological characteristics. Pediatr Radiol. 2015;45:1856-63.
- [CrossRef] [PubMed] [Google Scholar]
- Madelung deformity of the wrist managed conservatively. Cureus. 2020;12:e8225.
- [CrossRef] [Google Scholar]
- Volar ligament release and distal radius dome osteotomy for correction of Madelung's deformity. J Hand Surg Am. 2006;31:1499-506.
- [CrossRef] [PubMed] [Google Scholar]
- State of the art review: The pathogenesis and management of Madelung deformity. J Hand Surg Eur Vol. 2023;48:1116-25.
- [CrossRef] [PubMed] [Google Scholar]




