
Translate this page into:
Congenital bilateral radioulnar synostosis: A rare case report with review of literature

*Corresponding author: Aashay Sonkusale, Department of Orthopedics, Indira Gandhi Government Medical College and Hospital, Nagpur, Maharashtra, India. aashay49@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Sonkusale A, Gandhi P, Bharti L, Giri V. Congenital bilateral radioulnar synostosis: A rare case report with review of literature. Indian J Musculoskelet Radiol 2023;5:61-3.
Abstract
Congenital radioulnar synostosis (CRUS) is a rare anomaly of the upper limb which causes varying degrees of limitations in forearm rotations. It most commonly presents at the age of 6 years when the child starts going to school with difficulty in day-to-day activities. A 5-year-old male child presented to the outpatient department with complains of difficulty in forearm supination bilaterally. Plain radiography showed proximal radioulnar synostosis of 5 cm on both sides. He was managed conservatively with physiotherapy, occupational therapy, activity modification, and counseled about following up if no improvement occurred, in 2 years. CRUS can present as an isolated anomaly and is easily missed as it usually does not cause significant cosmetic concern and the child learns to overcome the deficits in forearm movements by compensatory movements at the shoulder and distal radioulnar joint. Diagnostic imaging plays a major role in identifying and planning management.
Keywords
Congenital
Radioulnar synostosis
Proximal
Rare

INTRODUCTION
Congenital radioulnar synostosis (CRUS) is a rare anomaly of the upper limb with about 400 cases reported worldwide.[1,2] It was first described by Sandifort in 1793. The average age of presentation is about 6 years when the child starts schooling and has difficulty in forearm rotations and restrictions in sports-related activities.[3] At about 4th week of gestation, the upper limb bud arises from the unsegmented body wall as a single outgrowth. The elbow joint starts appearing by the 5th week, with the radius and ulna sharing a common perichondrium by the 37th day and by the 7th week, the segmentation into radius and ulna as individual separate bones is complete. Any unfavorable insult during this period will lead to aberrations in segmentation resulting in varying degrees of radioulnar synostosis.[4]
CASE REPORT
A 5-year-old male child presented to the orthopedic outpatient department with mother being the informant complaining of limited range of motion at the elbow especially supination leading to difficulty in eating and washing his face. The mother had observed that the child also had trouble in holding powdered substances in his hands since earlier in childhood. Physical examination showed a deformation at elbow bilaterally with valgus of 20°. Supination was restricted to 110° on both sides; further, supination was possible only with compensatory external rotation at the shoulder [Figure 1]. Compensatory internal rotation was needed for full pronation on both sides [Figure 2]. Other movements at the elbow were within normal range. No hypermobility was noted at the wrist joints. No other skeletal abnormality was observed. Distal pulses were present and there was no neurodeficit present. The child was in good general condition with psychomotor development appropriate for his age. Family history was negative for similar afflictions. Routine hematogram was within normal limits.
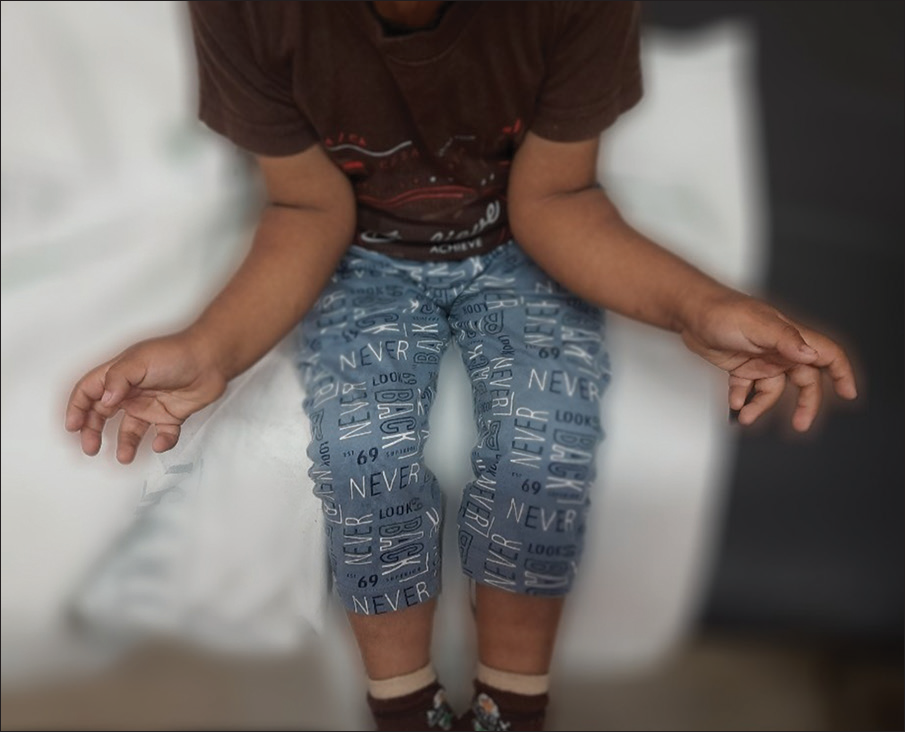
- Clinical photograph showing restricted supination bilaterally with further supination possible only after compensatory external rotation at shoulder.

- Clinical photograph showing full pronation possible only after compensatory internal rotation at shoulder.
Plain radiographs in anteroposterior and lateral views revealed radioulnar synostosis at both elbows of 5 cm on each side [Figures 3 and 4].
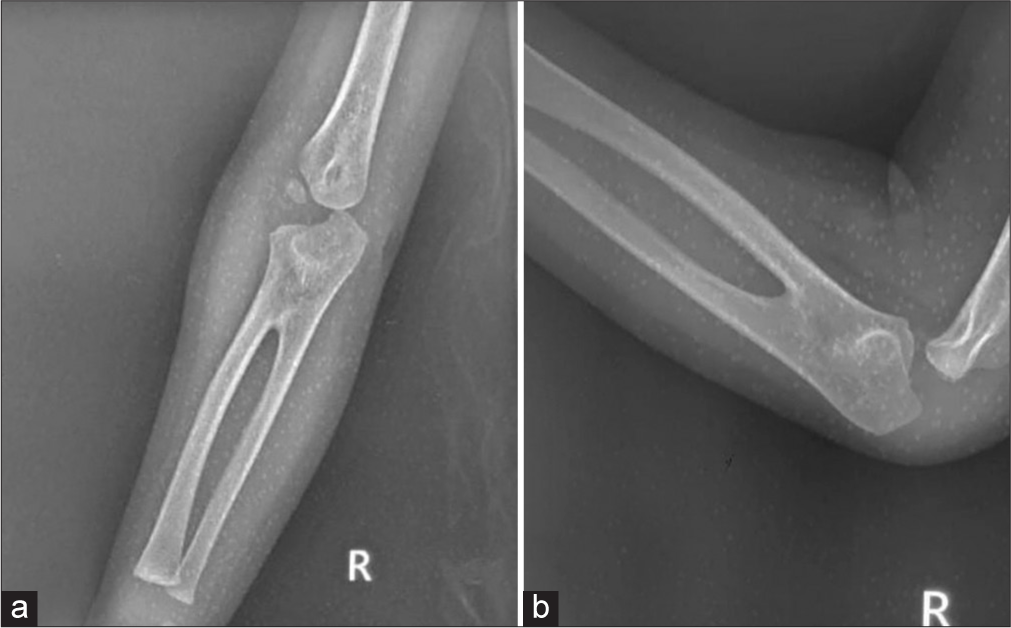
- Plain radiograph of the right elbow showing proximal radioulnar synostosis of 5 cm in anteroposterior view (a) and lateral view (b).
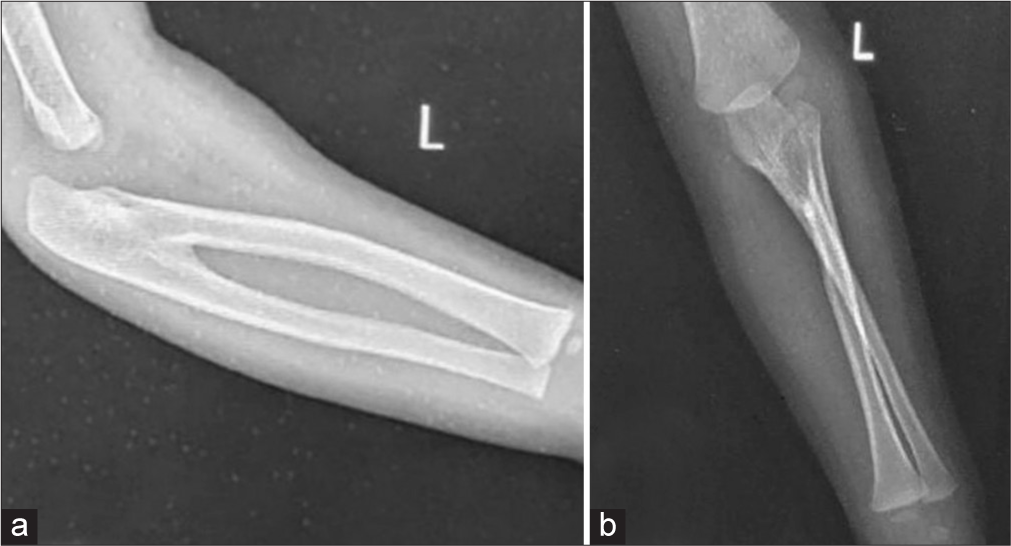
- Plain radiograph of the left elbow showing proximal radioulnar synostosis of 5 cm in anteroposterior (a) and lateral view (b).
DISCUSSION
CRUS is rare malformation which begins early in embryonic life resulting in varying degree of fusion of radius and ulna. It can also be acquired later in life due to secondary causes such as trauma and infection. CRUS is the most common congenital functional disorder of the elbow, found bilaterally in 60–80% of the cases.[5] It is often observed sporadically, but is familial in 9% of the cases having an autosomal dominant pattern of inheritance.[6] In 25% of the cases, it is genetically conditioned.[7] Radial abnormalities are associated with hematological disorders such as thrombocytopenia absent radius syndrome and fanconi anemia. Other associations include angelman syndrome, autism spectrum disorder, Poland’s syndrome, and polycystic kidney disorder.[8] The mean age of presentation is 6 years ranging from 6 months to 22 years – our case presented it at the age of 5 years.[3]
CRUS has been described on the basis of location of the synostosis, radiologic classification, and the functional impairment it causes. The most frequently used classification has been detailed by Cleary and Omer[9] into four types: Type 1 has no bony synostosis but with a smaller-sized radial head; type 2 has bony radioulnar synostosis; type 3 involves bony synostosis with posteriorly dislocated radial head; and type 4 emcompasses bony synostosis with anteriorly dislocated radial head. Our case can be classified as type 2 with proximal 5 cm of synostosis.
The management of CRUS depends on the functional impairment and can be conservative or operative. Cleary and Omer[9] who examined 36 elbows with CRUS prospectively, with none of them having any attempt at surgical correction and noted most of them had no major limitation as they were employed in jobs that required strenuous use of forearm. They found that the position of forearm did not affect the subjective degree of functional limitation and concluded that operative management was rarely indicated. Jia et al.[10] stated that recurrence is common following surgical treatment and soft-tissue changes need to be addressed if at all an osteotomy is planned. Conservative therapy is indicated in most cases as the growing child adapts to the position of forearm with movements at shoulder and distal radioulnar joint compensating limitations in forearm rotations. It requires a dedicated team of orthopedic surgeons, physiotherapists, and occupational therapists along with some activity modification. Surgical management includes rotational osteotomy and mobilization of synostosis and is often associated with complications such as compartment syndrome, neurological injury especially to posterior interosseous nerve, recurrence of malformation, and synostosis. Our patient was managed conservatively and was referred for physiotherapy. The mother was counseled about the abnormality and asked to return if there was no improvement.
CONCLUSION
CRUS is a rare anomaly and can often be isolated. It is easily missed as it does not cause a significant cosmetic concern when functional limitation is mild. Objective functional assessment and diagnostic imaging plays a key role in identifying and planning for management of these cases.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Financial support and sponsorship
Nil.
References
- Case report: Congenital radioulnar synostosis and its embryological correlation and functional assessment. J Anatomic Soc India. 2011;60:236-8.
- [CrossRef] [Google Scholar]
- Congenital radioulnar synostosis in an active duty soldier: Case report and literature review. Mil Med. 2000;165:425-8.
- [CrossRef] [PubMed] [Google Scholar]
- A case report of congenital bilateral proximal radioulnar synostosis in a 22-month-old child. West Afr J Radiol. 2019;26:50-2.
- [CrossRef] [Google Scholar]
- Congenital proximal radioulnar synostosis-a case report. Radiol Case Rep. 2020;15:1313-6.
- [CrossRef] [PubMed] [Google Scholar]
- Autosomal dominant and sporadic radio-ulnar syostosis. Am J Med Genet. 1997;68:127-34.
- [CrossRef] [Google Scholar]
- Congeniatal radioulnar synostisis. Study of a series of 37 children and adolescents. Chir Main. 1998;17:300-8.
- [CrossRef] [Google Scholar]
- Radioulnar synostosis and its hematology and genetic associations. Blood. 2010;116:2521.
- [CrossRef] [Google Scholar]
- Congenital proximal radio-ulnar synostosis. Natural history and functional assessment. J Bone Joint Surg Am. 1985;67:539-45.
- [CrossRef] [PubMed] [Google Scholar]
- Congenital unilateral proximal radioulnar synostosis: A surgical case report. Medicine (Baltimore). 2020;99:e19782.
- [CrossRef] [PubMed] [Google Scholar]




