
Translate this page into:
Decoding hip joint anatomy on radiographs and magnetic resonance imaging

*Corresponding author: Ritika Arunkumar Chamadia, Department of Radiology, Manipal Hospital, Pune, Maharashtra, India. ritikachamadia@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Chamadia RA, Agarwal E, Lokhande P. Decoding hip joint anatomy on radiographs and magnetic resonance imaging. Indian J Musculoskelet Radiol. 2025;7:3-12. doi: 10.25259/IJMSR_2_2025
Abstract
Knowledge of the anatomy of the human body is vital before we proceed with the abnormalities. Similarly, before we dive right into imaging the hip pathologies, this article briefly reviews the hip joint anatomy on radiographs and magnetic resonance imaging through this pictorial assay, which includes bones, joints, muscles, tendons, ligaments, neurovascular bundles, and adjacent supporting structures.
Keywords
Hip joint anatomy
Magnetic resonance imaging
Radiographs

INTRODUCTION
The hip joint is the articulation between the acetabulum and the head of the femur and is a ball-and-socket type of diarthrodial joint with osseous components primarily dictating its inherent stability.
Radiographs are the primary imaging modality for evaluating the bony pelvis and hip, followed by computed tomography. However, for the evaluation of the adjacent soft tissue, magnetic resonance imaging (MRI) is the gold standard.
Learning objectives
This pictorial essay aims to provide insight into imaging of hip joint anatomy using radiographs and MRI.
Magnetic resonance (MR), with its inherent improvement in soft-tissue delineation, provides accurate delineation of the underlying structures.
OSSEOUS STRUCTURES
The acetabulum is formed as a junction of the three pelvic bones (approximates the surface of two-thirds of a sphere) with contributions from the ilium, ischium, and pubis [Figure 1a].[1]
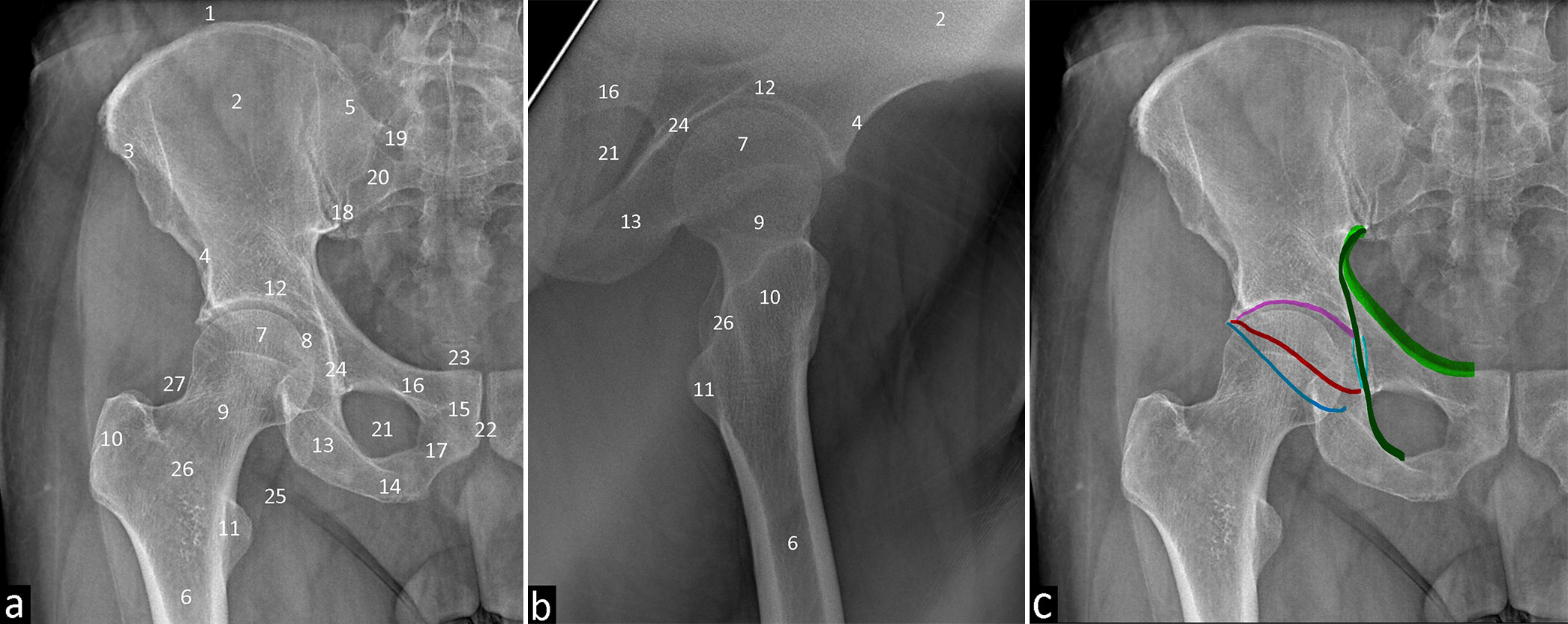
- Radiographs of the Hip (a) Frontal projection 1. Iliac crest. 2. Ilium. 3. Anterior superior iliac spine. 4. Anterior inferior iliac spine. 5. Posterior superior iliac spine. 6. Femur. 7. Femoral head. 8. Fovea centralis. 9. Femoral neck. 10. Greater trochanter. 11. Lesser trochanter. 12. Acetabulum. 13. Ischium. 14. Ischial tuberosity. 15. Pubis. 16. Superior pubic ramus. 17. Inferior pubic ramus. 18. Sacroiliac joint. 19. Sacral Arcuate lines. 20. Anterior sacral foramina. 21. Obturator foramen. 22. Symphysis pubis. 23. Coccyx 24. Koehler’s teardrop 25. Psoas fat pad 26. Intertrochanteric crest 27. Gluteal fat pad, (b) Lateral projection 2. Ilium. 4. Anterior inferior iliac spine. 6. Femur. 7. Femoral head. 9. Femoral neck. 10. Greater trochanter. 11. Lesser trochanter. 13. Ischium. 16. Superior pubic ramus. 21. Obturator foramen. 24. Koehler’s teardrop. 26. Intertrochanteric crest. (c) Frontal projection demonstrating important lines which are color coded. Light broad green- iliopubic line. Dark thin green- ilioischial line. Pink- Acetabular roof. Red-Anterior acetabular wall. Dark blue-Posterior acetabular wall. Light blue curved-Koehler’s teardrop.
It is incomplete in its inferior portion; completed by the transverse acetabular ligament along the inferior margin forming the “socket,” that holds the femoral head [Figure 1b] (“ball”) in position.[2]
The iliopubic line [ Figure 1c] extends from the medial margin of the iliac wing, along the superior margin of the superior pubic ramus, to the pubic symphysis delineating the anterior column of the pelvis.
The ilioischial line [Figure 1c] also starts from the medial margin of the iliac wing and extends to the ischial tuberosity along the ischial bone delineating the posterior column.
Sacral arcuate lines [Figure 1a, label 19] should be smooth and symmetrical; discontinuity may indicate sacral fractures. These define the inferior margin of the costal element that forms the anterior sacral canal roof and neural groove.
Shenton arc or line runs along the inferior margin of the superior pubic ramus and the inferior and medial surface of the femoral neck. Its interruption indicates the presence of a femoral neck fracture or developmental dysplasia of the hip.[3]
The gluteal fat stripe [Figure 1b] runs along the superior portion of the neck of the femur and denotes the fat between the gluteal minimus tendon and the ischiofemoral ligament. The iliopsoas fat stripe is the lucency seen immediately adjacent to the iliopsoas tendon. These stripes bulge away from the neck of the femur or become effaced if a joint effusion is present in the hip.[4]
The acetabular roof [Figure 1c] is the superior weight-bearing portion of the acetabulum, which includes parts of both columns. Flattening of the roof occurs in achondroplasia. The medial wall of the acetabulum is normally lateral to the ilioischial line. The anterior acetabular wall is the anterior acetabulum rim, which runs medial to the posterior acetabular wall. Similarly, the posterior acetabular wall is the posterior rim, which runs lateral to the anterior wall. These lines should never cross.[5]
Synovial herniation pits (pitt pits)
These are round or oval radiolucencies located subchondrally or subcortically with thin sclerotic margins found on the anterosuperior femoral neck. These are associated with repetitive impingement or pressure during hip flexion and rotation and are indicative of femoroacetabular impingement, a key factor contributor to early hip osteoarthritis.[6]
Os Acetabuli
Os acetabuli are unfused accessory ossification centers along the acetabular rim. They may result from the persistence of secondary ossification centers, incomplete healing of acetabular rim fractures, or ossification in the labrum. These structures can contribute to acetabular rim impingement or compromise joint stability. Imaging typically reveals small ossicles surrounded by hyaline cartilage.[6]
Marrow
Normal bone marrow is of two types: Red (hematopoietic) marrow and yellow (inactive) marrow, which differ in composition and hence MRI appearances. After infancy, red marrow gradually converts to yellow marrow, starting in the peripheral/appendicular skeleton and moving to the central (axial skeleton) regions. In long bones, this transition occurs from the diaphysis to the metaphysis, with the epiphysis and apophysis converting first, typically within the first 10 years of life. In adults, residual red marrow is found in well-vascularized areas such as the metaphysis of long bones and adjacent to vertebral endplates.[7]
The proximal femoral epiphysis and apophysis contain yellow marrow, displaying fat-like signal intensity on all MRI sequences. In contrast, the bony pelvis, femoral neck, and intertrochanteric region typically contain red marrow, which appears on T1-weighted images with signal intensity lower than fat or yellow marrow but higher than skeletal muscle.[1]
Cartilage
The acetabular rim is lined by articular cartilage called the “lunate.” It is horse-shoe shaped.[2] Cartilage is radiolucent on radiographs, making it appear invisible within the joint space; the joint space seen on radiographs represents the gap between opposing bones filled with cartilage and synovial fluid, rather than the cartilage itself.
The acetabular fossa is the central depression in the acetabulum where the cartilage lining is absent. Fibrofatty tissue is present in the fossa and is lined by synovium.[2,8]
Normal articular cartilage on MRI is characterized by distinct layers of varying signal intensities. When oriented perpendicular to the main magnetic field (B0), these layers include a low-signal-intensity surface, a high-signal-intensity transitional layer, and a low-signal-intensity deep layer near the subchondral bone. These variations reflect continuous changes in T2 relaxation times across cartilage thickness, which are minimally influenced by T1 relaxation, diffusion, or proton density. The shortest T2 relaxation time, around 10 ms, makes T2 the primary determinant of tissue contrast on most MRI sequences. The phenomenon of T2 anisotropy, influenced by the magic-angle effect at approximately 54.7° relative to B0, adds to the layered appearance of cartilage.[9]
Histologically, the MRI layers correspond to cartilage zones with distinct collagen fibril orientations. Collagen fibrils are horizontal in the superficial zone, perpendicular in the deep zone, and randomly oriented in the transitional zone. This organization accounts for T2 heterogeneity and anisotropy seen on MRI. Macroscopic structure, such as fibers and layers, also contributes to MRI appearance. These structures radiate from the subchondral bone and curve into the articular surface, explaining the variations in T2 relaxation times and anisotropy across cartilage. Joint-specific differences in cartilage architecture further influence MRI findings, making it challenging to standardize imaging protocols for evaluating cartilage integrity.[9]
Advanced MRI techniques for cartilage assessment
Several advanced MRI pulse sequences optimize the evaluation of articular cartilage. Three-dimensional T1-weighted spoiled gradient recalled echo (SPGR) imaging provides high-resolution, contiguous thin-slice images with strong contrast between cartilage and adjacent tissues.
Fat-suppressed SPGR imaging enhances dynamic range, allowing for better detection of subtle cartilage abnormalities. However, longer acquisition times and sensitivity to artifacts are limitations.
Fast spin-echo imaging offers rapid acquisition with high resolution. It benefits from inherent magnetization transfer effects, which enhance the conspicuity of cartilage abnormalities- particularly effective for detecting cartilage defects and assessing other joint structures like ligaments and menisci.
Limitations include reduced through-plane resolution and potential image blurring. In addition, MR arthrography, particularly indirect techniques, is valuable for evaluating cartilage repair, as it highlights the surface and defects of repair tissue.[9]
Supraacetabular Fossa is present at the 12 o’clock position of the acetabular roof.
Types: Type 1: Filled with contrast. Type 2: Filled with cartilage. Can mimic cartilage defects but differs in location and marrow signal.[6]
Stellate crease is a focal area deficient in hyaline cartilage within the acetabular roof. Located medial to the supraacetabular fossa and continuous with the acetabular notch.[6]
MUSCLES AND TENDONS
Normal skeletal muscle is intermediate in signal intensity on all pulse sequences. T1-weighted MRIs are best for evaluating muscle bulk and signal intensity. In these images, muscles have a “marbled” appearance because of high signal-intensity fat located between intermediate signal-intensity muscles and interspersed between fibers of individual muscles. The appearance of fatty infiltration ranges from high T1 signal intensity marbling to complete high T1 signal intensity replacement [Table 1].[1]
| Muscle groups | Muscles | Origin | Insertion |
|---|---|---|---|
| Adductors | Pectineus [Figures 2-4, label 1] | Pectineal line of the pubis | Pectineal line (oblique) - base of the lesser trochanter to linea aspera on the posterior aspect of the femur |
| Adductor brevis [Figures 2-4, label 2] | Outer surface of body of pubis and inferior ramus of the pubic bone | proximal portion of linea aspera | |
| Adductor longus, [Figures 2-4, label 3] | Body of pubis (lateral to the pubic symphysis and inferior to the crest) | Linea aspera- in its Middle 1/3rd | |
| Adductor magnus [Figures 2-4, label 4] Adductor part: Hamstring part: | Ischiopubic ramus Ischial tuberosity | Proximal femur (Posterior), Linea aspera, Medial supracondylar line Adductor tubercle | |
| Gracilis [Figures 2-4, label 5] | External surface of the body of the pubis, Inferior pubic ramus, Ischial ramus | Part of the pes anserinus tendon onto the medial aspect of the proximal tibia | |
| Abductors | Gluteus medius [Figures 2-4, label 13] | Ilium between the posterior and anterior gluteal line along the gluteal surface, Gluteal aponeurosis, Iliac crest (posteroinferior) | Greater trochanter -Postero-superior and lateral facet[1] |
| Gluteus minimus [Figures 2-4, label 14] | Ilium between the anterior and inferior gluteal lines along the gluteal surface | Greater trochanter -Anterior facet[1] | |
| Tensor fascia lata [Figures 2-4, label 18] | ASIS- anterior aspect | Iliotibial tract of fascia lata- anterolateral tibia. | |
| Sartorius [Figures 2-4, label 19] | ASIS | Proximal tibia - medial aspect (Part of the pes anserinus tendon) | |
| External rotators | Piriformis [Figures 2-4, label 10] | Sacrum- anterolateral surface | Greater trochanter |
| Quadratus femorus [Figures 2-4, label 11] | Ischium- lateral portion, anterior to the ischial tuberosity | Quadrate tubercle on the intertrochanteric crest of the femur | |
| Obturator internus, [Figures 2-4, label 7] | Internal surface of obturator membrane and deep surfaces of pubic bone and ischium, Anterolateral wall of pelvis | Greater trochanter- Medial aspect | |
| Gemelli superior: [Figures 2-4, label 8] Inferior: [Figures 2-4, label 9] | Ischial spine- Gluteal surface Ischial tuberosity- Upper aspect | Trochanteric fossa- Middle Greater trochanter (Medial side) and obturator internus tendon (inferior surface) | |
| Extensors-Hamstrings | Gluteus maximus | Ilium- Gluteal surface behind the | Iliotibial band, Gluteal |
| [Figures 2-4, label 12] | posterior gluteal line, Lumbar fascia, Lateral mass of sacrum, Sacrotuberous ligament | tuberosity- proximal femur (posterior aspect)[1] | |
| Semimembranosus [Figures 2-4, label 15] | Ischial tuberosity -(Superolateral portion)[1] | Infraglenoid tubercle- tibial condyle, Posterior joint capsule, Popliteal fascia, Posterior horn of medial meniscus | |
| Long head of Biceps femoris [Figures 2-4, label 16] | As conjoint tendon -ischial tuberosity (Inferomedial facet)[1] | Fibular head, Lateral tibial condyle, Crural fascia, | |
| Semitendinosus [Figures 2-4, label 17] | Proximal tibia - medial aspect (Part of the pes anserinus tendon) | ||
| Flexors- | Sartorius, [Figures 2-4, label 19] | ASIS[1] | Proximal tibia - medial aspect (Part of the pes anserinus tendon) |
| Rectus femorus, [Figures 2-4, label 20] | direct/straight head- AIIS, Indirect/reflected in - superior acetabular rim[1] | Quadriceps tendon | |
| Psoas major: [Figures 2-4, label 22] | Vertebral bodies-T12 to L5 | Lesser trochanter[1] | |
| Psoas minor: | T12 and L1 | Iliopubic eminence | |
| Iliacus. [Figures 2-4, label 21] | Lesser trochanter[1] |
ASIS: Anterosuperior iliac spine, AIIS: Anterior inferior iliac spine
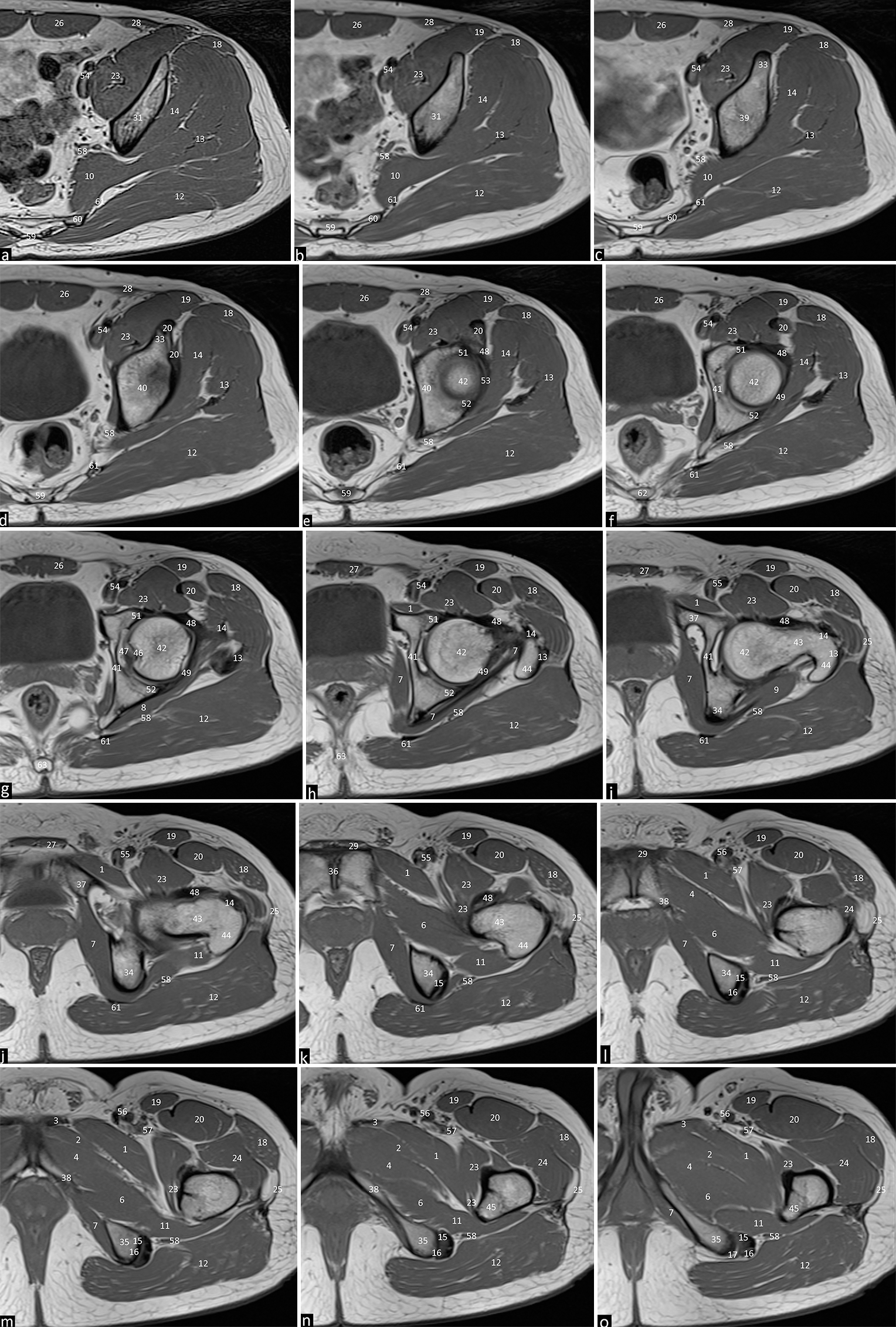
- Axial T1 weighted images of the left hip joint depicting the normal anatomical structures from Cranial to caudal with subpart images. (a-o) 1. Pectineus. 2. Adductor brevis. 3. Adductor longus. 4. Adductor magnus. 5. Gracilis. 6. Obturator externus. 7. Obturator internus. 8. Superior gemellus. 9. Inferior gemellus. 10. Piriformis. 11. Quadratus femorus. 12. Gluteus maximus. 13. Gluteus medius 14. Gluteus minimus. 15. Semimembranosus. 16. Long head of biceps femoris. 17. Semitendinosus. 18. Tensor fascia lata. 19. Sartorius. 20. Rectus femorus. 21. Iliacus. 22. Psoas major. 23. Iliopsoas. 24. Vastus lateralis. 25. Iliotibial tract. 26. Rectus abdominus. 27. Pyramidalis muscle. 28. Abdominal oblique muscle. 29. Rectus aponeurosis. 30. Coccygeus. 31. Ilium. 32. Anterior superior iliac spine. 33. Anterior inferior iliac spine. 34. Ischium. 35. Ischial tuberosity. 36. Pubic symphysis. 37. Superior pubic ramus. 38. Inferior pubic ramus. 39. Acetabulum. 40. Acetabular roof. 41. Acetabular fossa. 42. Femoral head. 43. Femoral neck. 44. Greater trochanter. 45. Lesser trochanter. 46. Fovea centralis. 47. Ligamentum teres. 48. Iliofemoral ligament. 49. Ischiofemoral ligament. 50. Pubofemoral ligament. 51. Anterior labrum. 52. Posterior labrum. 53. Acetabular labrum. 54. External iliac artery and vein. 55. Common femoral artery and vein. 56. Superficial femoral artery and vein. 57. Profunda femoral artery and vein. 58. Sciatic nerve 59. Sacrum. 60. Sacral ala 61. Sacrotuberous ligament. 62. Sacrococcygeal junction. 63. Coccyx.
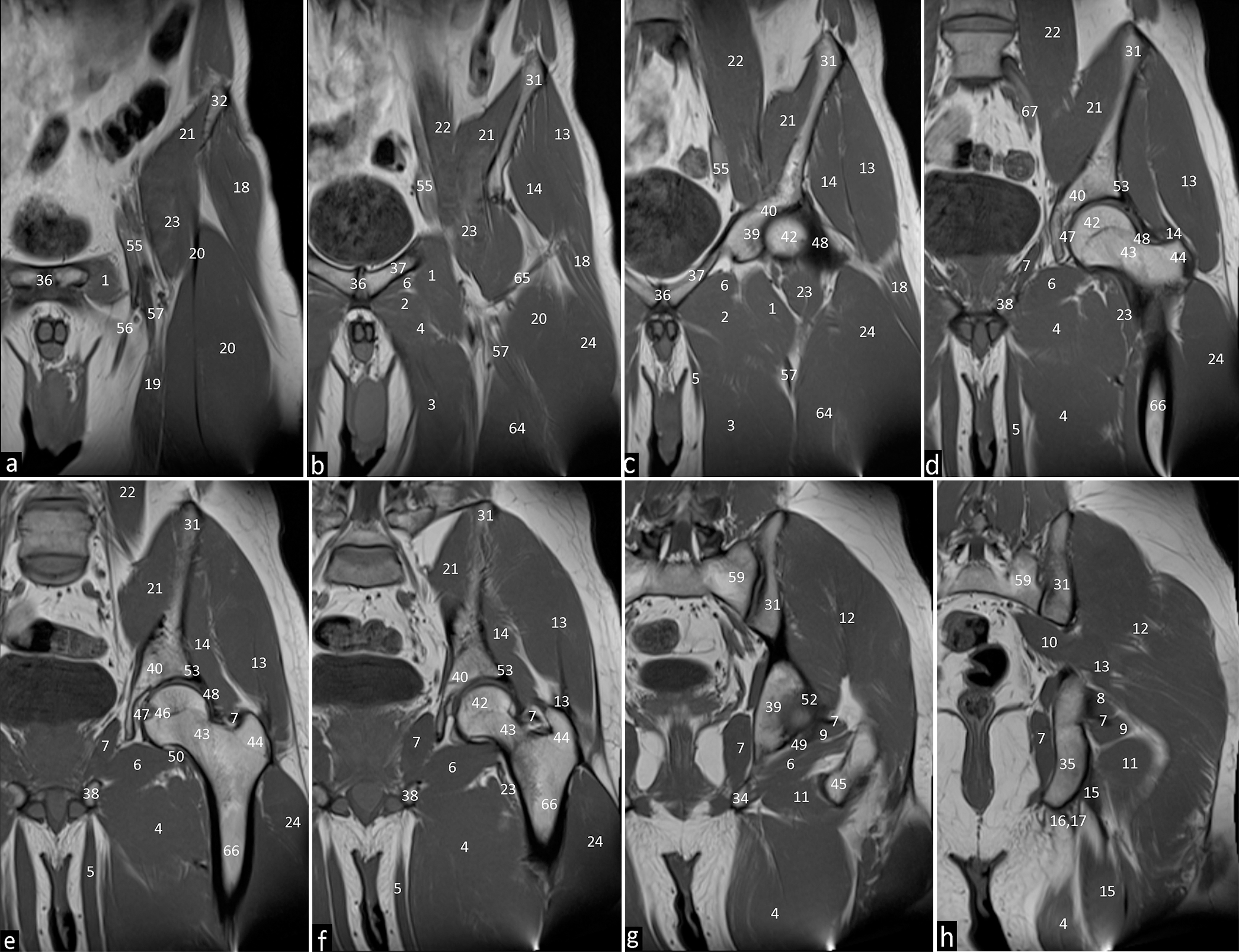
- Coronal T1 weighted images of the left hip joint depicting the normal anatomical structures from to anterior to posterior with subpart images. (a-h) 1. Pectineus. 2. Adductor brevis. 3. Adductor longus. 4. Adductor magnus. 5. Gracilis. 6. Obturator externus. 7. Obturator internus. 8. Superior gemellus. 9. Inferior gemellus. 10. Piriformis. 11. Quadratus femorus. 12. Gluteus maximus. 13. Gluteus medius. 14. Gluteus minimus. 15. Semimembranosus. 16. Long head of biceps femoris. 17. Semitendinosus. 18. Tensor fascia lata. 19. Sartorius. 20. Rectus femorus. 21. Iliacus. 22. Psoas major. 23. Iliopsoas. 24. Vastus lateralis. 31. Ilium. 32. Anterior superior iliac spine. 35. Ischial tuberosity. 36. Pubic symphysis. 37. Superior pubic ramus. 38. Inferior pubic ramus. 39. Acetabulum. 40. Acetabular roof. 42. Femoral head. 43. Femoral neck. 44. Greater trochanter. 46. Fovea centralis. 47. Ligamentum teres. 48. Iliofemoral ligament. 49. Ischiofemoral ligament. 50. Pubofemoral ligament. 53. Acetabular labrum. 55. Common femoral artery and vein. 56. Superficial femoral artery and vein. 57. Profunda femoral artery and vein. 59. Sacrum. 64. Vastus intermedius. 65. Lateral circumflex femoral artery. 66. Femoral shaft. 67. External iliac vessels.
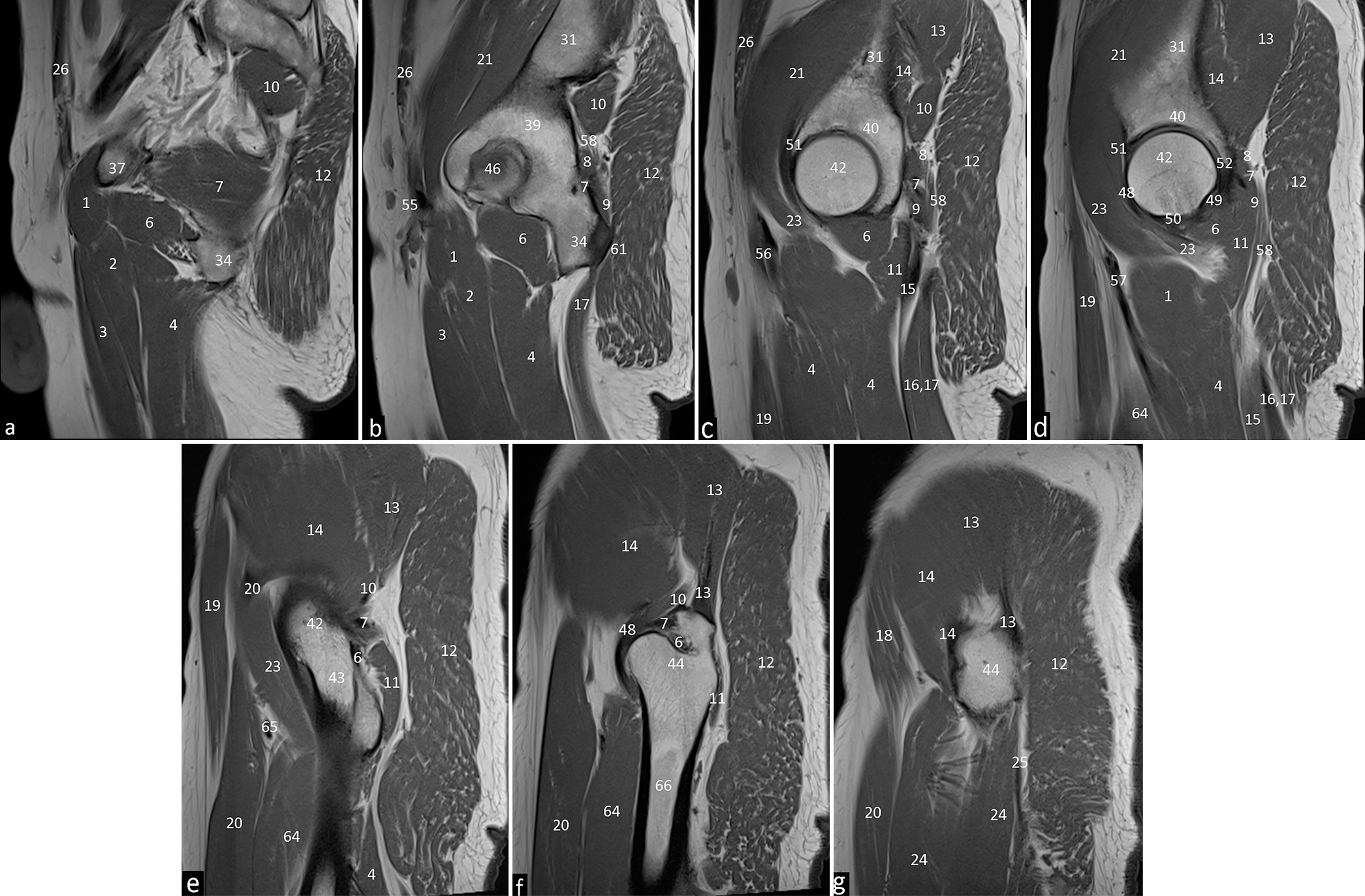
- T1 weighted sagittal images of the left hip joint depicting the normal anatomical structures from medial to lateral with subpart images (a-g) 1. Pectineus. 2. Adductor brevis. 3. Adductor longus. 4. Adductor magnus. 6. Obturator externus. 7. Obturator internus. 8. Superior gemellus. 9. Inferior gemellus. 10. Piriformis. 11. Quadratus femorus. 12. Gluteus maximus. 13. Gluteus medius. 14. Gluteus minimus. 15. Semimembranosus. 16. Long head of biceps femoris. 17. Semitendinosus. 18. Tensor fascia lata. 19. Sartorius. 20. Rectus femorus. 21. Iliacus. 23. Iliopsoas. 24. Vastus lateralis. 25. Iliotibial tract. 26. Rectus abdominus. 31. Ilium. 34. Ischium. 37. Superior pubic ramus. 39. Acetabulum. 40. Acetabular roof. 42. Femoral head. 43. Femoral neck. 44. Greater trochanter. 46. Fovea centralis. 48. Iliofemoral ligament. 51. Anterior labrum. 55. Common femoral artery and vein. 56. Superficial femoral artery and vein. 58. Sciatic nerve. 61. Sacrotuberous ligament. 64. Vastus intermedius. 65. Lateral circumflex femoral artery. 66. Femoral shaft. 67. External iliac vessels.
The MRI appearance of tendons is determined by their structural properties and relaxation times.
Tendons, composed of aligned collagen and water molecules, have a very short T2 relaxation time (1–2 ms), causing them to appear as low-signal-intensity structures on conventional imaging sequences.
This low signal intensity is angle-dependent, with T2 increasing at angles above 20° to the magnetic field and peaking at 55°—the “magic angle.” Longer echo times can mitigate magic angle effects, with critical thresholds varying by sequence type (e.g., 30 ms for gradient echo, 40 ms for spin echo, and 70 ms for fast-spin echo).
T1 relaxation times in tendons are also short (~600 ms at 3T), and conventional sequences primarily detect signals when T2 is significantly increased, effectively making them T2-weighted for tendons.[10]
Accessory Iliacus Tendon- A thin intramuscular tendon within the lateral iliacus muscle. Can mimic iliopsoas tendon tears but appears distinct on fat-suppressed imaging.[6]
BURSA
Small fluid-filled synovial-lined sacs that reduce the pressure in and around the joints reducing friction in areas where tendons glide over bony surfaces or move against each other. Bursae are classified by location into subcutaneous, subfascial, subtendinous, and submucosal types. They can also be categorized as communicating or noncommunicating based on their relationship with nearby joints. Communicating bursae, such as the iliopsoas bursa near the hip, share a synovial connection with adjacent joints. Most bursae are potential spaces and are not typically visible on imaging under normal conditions [Table 2].[11-13]
| Name of the bursa | Relations |
|---|---|
| Greater trochanteric | 3 parts – deep to each of the 3 gluteal tendons |
| Iliopsoas | Anterolateraly- Iliopsoas muscle, Anteriorly/anteromedially- Femoral vessels, Medially- Pectineal eminence of the pubic bone, Posteriorly- Joint capsule and labrum. |
| Ischiogluteal | Posterior and inferior - ischial tuberosity Deep to the inferior portion of the gluteus maximus muscle |
Iliopsoas bursa
The largest bursa around the hip. It lies beneath the musculotendinous portion of the iliopsoas muscle, anterior to the joint capsule, and lateral to the femoral vessels.
Normally collapsed, the bursa can become distended due to excessive synovial fluid production, often resulting from increased intraarticular pressure in conditions such as arthritic hips. Associated diseases include trauma, osteoarthritis, avascular necrosis, rheumatoid arthritis, synovial chondromatosis, pigmented villonodular synovitis, gout, and infection.
Differential diagnoses for an enlarged iliopsoas bursa include hernias, neoplasms, lymphadenopathy, undescended testes, hematomas, psoas abscesses, femoral aneurysms, and arteriovenous fistulas.[12]
Obturator externus bursa
A potential space found between the obturator externus tendon and the ischiofemoral capsular ligaments at the back of the hip joint capsule. It is connected to the hip joint in all cases and is sometimes regarded as an articular recess rather than a true bursa. On MRI, the bursa can accumulate intraarticular bodies and joint fluid. MR arthrography can expand the capsule and fill the bursa with contrast, which should not be confused with a tear or rupture of the joint capsule.[14]
Trochanteric bursa
One of the major bursae near the greater trochanter. It is the largest and covers the posterior facet beneath the gluteus medius tendon and proximal vastus lateralis insertion. Positioned beneath the gluteus maximus muscle and the iliotibial tract, it does not extend over the anterior border of the lateral facet. On non-enhanced coronal MRI, it appears as a fine linear structure paralleling the posterior facet. Trochanteric bursitis is a common cause of hip pain, often linked to obesity, trauma, inflammatory arthritis, or total hip arthroplasty.[12]
Peritrochanteric edema
Seen in patients with lateral hip pain, but it doesn’t necessarily correlate with the pain itself. It is common in older patients and often bilateral. This edema may represent an early, asymptomatic stage of hip pathology.
In older patients, particularly when it occurs alone, it should be considered a benign finding and not linked to greater trochanteric pain syndrome. While conditions like greater trochanteric pain syndrome, bursitis, and gluteal tendon issues are linked to lateral hip pain, peritrochanteric edema seen as increased T2-weighted signal on MRI without actual fluid buildup—does not directly contribute to the pain.[14]
Subgluteus medius bursa
This bursa is located deep in the distal gluteus medius tendon, covering the superior part of the lateral facet. Its superior boundary aligns with the tip of the trochanter, the anterior boundary with the lateral facet, and the posterior and inferior boundaries with the gluteus medius tendon insertion.[12]
Subgluteus minimus bursa
Found in the region of the anterior facet, lies beneath the gluteus minimus tendon, positioned medial and superior to its insertion.[12]
LIGAMENTS AND CAPSULE
MRI appearance of ligaments similar to tendons is determined by their structural properties and relaxation times. Ligaments, with a slightly higher T2 share a similar low-signal appearance on both T1- and T2-weighted sequences due to their structural similarities to tendons [Table 3].[1,10,11,15]
| Ligaments | Origin | Insertion |
|---|---|---|
| Teres femoris | Fovea | Transverse acetabular ligament |
| Iliofemoral (Y-shaped, strongest) | AIIS and the superior acetabulum | Intertrochanteric line |
| [Figures 2-4, label 48] | ||
| Ischiofemoral [Figures 2-4, label 49] | Ischium Acetabulum (posteroinferior) | Greater trochanter -medial base Femoral neck -superolateral aspect |
| Pubofemoral [Figures 2-4, label 50] | Pubic bone- pectineal eminence, obturator crest, Superior pubic ramus, Obturator membrane | Lesser trochanter, medial to the attachment of iliofemoral ligament |
These ligaments are thickenings that reinforce the joint capsule and assist stabilization of hip joint [Figures 2-4, labels 47-50].
A circular band of fibers, known as the zona orbicularis, forms a collar around the femoral neck at its base. This structure integrates with the fibers of the iliofemoral and ischiofemoral ligaments without directly attaching to bone.[1,16]
Ligamentum Teres [Figures 2-4, label 47]- Hip stabilizer, during abduction, flexion, and external rotation. A cord-like, hypointense structure on MRI. Thickening, hypertrophy, or absence is seen in developmental dysplasia of the hip.[6]
Plicae- Synovial folds that may stabilize the joint but are generally asymptomatic. They are located adjacent to the acetabular labrum, femoral neck, and at the acetabular base of the ligament of the femur.[6]
Pectinofoveal Fold- A retinaculum extending from the lesser trochanter to the fovea capitis. Seen on MR arthrograms, it should not be mistaken for a plica. Contains important arterial branches.[6]
LABRUM
The labrum [Figures 2-4, Labels 51-53] is a fibrocartilaginous structure that attaches to the rim of the acetabulum, analogous to the labral attachment to the glenoid rim in the shoulder. It is hypointense on all sequences. However, only encircles 3/4th of the circumference.[2]
Sublabral sulcus is a normal variant, characterized by a linear high T2-weighted signal located at the chondrolabral junction, commonly appearing in the posteroinferior or anterosuperior regions. It undermines the labrum and is normally smooth-edged without full-thickness involvement. Distinguishing a sublabral sulcus from a labral tear is important, as a tear is usually located in the anterosuperior labrum, associated with clinical symptoms, and can be relieved with an intra-articular anesthetic.[14]
Perilabral sulcus is a normal space between the labrum and the joint capsule, most visible in the superior joint space, apparent when the joint is distended, such as during MR arthrography, and can sometimes mimic a paralabral cyst when fluid is trapped in the recess. A large sulcus might resemble capsular stripping.[14]
NEUROVASCULAR STRUCTURES
On MRI, nerves typically appear round or oval in cross-section, with a stippled or honeycombed pattern. This stippling reflects the nerve fascicles, which are separated by varying amounts of fat, and is known as the “fascicular pattern.” The fascicles generally show similar or slightly higher signal intensity compared to skeletal muscle on T2-weighted images. They are uniform in size, giving larger nerves, like the sciatic, a striated appearance when viewed longitudinally [Table 4].[1,10,16,17]
| Nerve | Roots | Course | Other information |
|---|---|---|---|
| Sciatic nerve [Figures 2-4, label 58] | L2 to S3 | Pierces the piriformis; exits dorsally via the sciatic notch; courses deep to the gluteus maximus | Large nerve in close relation to the pyriform on axials in the posterior thigh. |
| Femoral nerve | L2 to L4 | Lateral border of the inferior psoas muscle, before descending between the psoas (lateral border) and iliacus (medial border) muscles. | Is seen along with femoral vessels in the anterior thigh. |
| Obturator nerve | L2 to L4 | Anterior to the iliopsoas; passes dorsal to the common iliac arteries; travels along the lateral wall of the pelvis; exits the pelvis through the obturator canal | |
| Vessels | Branches | Supplies | |
| Common femoral artery [Figures 2-4, label 55] | Superficial [Figures 2-4, label 56] | Continues caudally and supplies the lower limb upto the foot | |
| Profunda [Figures 2-4, label 57] | Thigh muscles |
Sciatic nerve
Supplies motor function to the hamstring muscles and part of the adductor magnus. Both motor and sensory functions to the leg and foot are via the tibial and common peroneal nerves, which are branches of the sciatic nerve. Compression of the nerve is diagnosed typically through MRI. Causes include trauma, mass lesions, or conditions like piriformis syndrome, which causes nerve irritation or compression at the greater sciatic foramen.[18]
Femoral nerve
It innervates the flexors of the hip and extensors of the knee, as well as provides sensory supply to the anterior portion of the thigh and medial portion of the leg through the saphenous nerve.
Neuropathy can occur due to compression, trauma, or surgical injury, resulting in paraesthesia in the thigh, leg, and foot. MRI findings include increased nerve size and signal intensity, along with any mass lesions that may cause nerve compression. Nerve, artery, vein, and lymphatics lie from lateral to medial at the level of the head of the femur.[18]
Obturator nerve
It provides sensory supply to the medial portion of the thigh and motor supply to adductor muscles. MRI is used to detect lesions and denervation changes in the nerve, helping identify entrapment or mass effects. It can be entrapped in the obturator canal due to trauma, cysts, or surgical complications. In athletes, it may result from chronic adductor tendinopathy.[18]
CONCLUSION
It is prudent to have anatomical knowledge of the hip and to understand the imaging anatomy optimally for a reporting radiologist. The above article states salient imaging features of the normal complex hip joint in adults in a different style using mainly tables and images for access and ease of review in day-to-day practice.
Acknowledgment
I extend my heartfelt thanks to Dr. Raj Chari, Dr. Stanzin Spalkit, my seniors and Dr. Sanjay Desai my mentor for their guidance and support throughout the development of this article. Their expertise and feedback were invaluable and I am deeply grateful for their mentorship.
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Conflict of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship: Nil.
References
- MR imaging of normal hip anatomy. Magn Reson Imaging Clin N Am. 2013;21:1-19.
- [CrossRef] [PubMed] [Google Scholar]
- Magnetic resonance imaging of the hip. J Magn Reson Imaging. 2008;27:435-45.
- [CrossRef] [PubMed] [Google Scholar]
- Diagnosis and treatment of slipped capital femoral epiphysis: Recent trends to note. J Orthop Sci. 2018;23:220-8.
- [CrossRef] [PubMed] [Google Scholar]
- The pelvic radiograph: Lines, arcs and stripes. Singapore Med J. 2021;62:333-40.
- [CrossRef] [PubMed] [Google Scholar]
- Hip anatomic variants that may mimic pathologic entities on MRI: Nonlabral variants. AJR Am J Roentgenol. 2013;201:W401-8.
- [CrossRef] [PubMed] [Google Scholar]
- Bone marrow lesions: A systematic diagnostic approach. Indian J Radiol Imaging. 2014;24:279-87.
- [CrossRef] [PubMed] [Google Scholar]
- From the RSNA refresher courses. Radiological society of North America. Chronic adult hip pain: MR arthrography of the hip. Radiographics. 2000;20:S43-52.
- [CrossRef] [PubMed] [Google Scholar]
- MRI of articular cartilage: revisiting current status and future directions. AJR Am J Roentgenol. 2005;185:899-914.
- [CrossRef] [PubMed] [Google Scholar]
- Gray's anatomy: The anatomical basis of clinical practice (40th ed). Madrid, Spain: Churchill Livingstone; 2008.
- [Google Scholar]
- Imaging of hip disorders in athletes. Radiol Clin North Am. 2002;40:267-87. vi-vii
- [CrossRef] [PubMed] [Google Scholar]
- MR imaging of the hip: Avoiding pitfalls, identifying normal variants. Appl Radiol Oncol. 2018;12:8-14.
- [CrossRef] [Google Scholar]
- Operative hip arthroscopy (2nd ed). New York: Springer Science and Business Media; 2005.
- [Google Scholar]
- Essential clinical anatomy (4th ed). Baltimore, MD: Lippincott Williams and Wilkins; 2011.
- [Google Scholar]
- Nerve entrapment syndromes of the lower limb: A pictorial review. Insights Imaging. 2023;14:166.
- [CrossRef] [PubMed] [Google Scholar]




