
Translate this page into:
Expanded Goldenhar Complex with Multiple Rare Syndromic Associations

*Corresponding author: Sunitha Vellathussery Chakkalakkoombil, Department of Radiodiagnosis, JIPMER, Pondicherry, India. drsunithapnair@rediffmail.com
-
Received: ,
Accepted: ,
How to cite this article: Mohan SL, Chakkalakkoombil SV, Deekonda S, Mohapatra DP. Expanded Goldenhar Complex with Multiple Rare Syndromic Associations. Indian J Musculoskelet Radiol 2020;2(2):144-8.
Abstract
Goldenhar syndrome (GS) is the most severe form of the oculoauriculovertebral spectrum, a developmental disorder primarily involving the structures derived from the first and second branchial arches, intervening first pharyngeal pouch and branchial cleft characterized by microtia, facial asymmetry, ocular abnormalities, and abnormalities of the vertebral column. A multifactorial etiology involving genetic and environmental factors has been proposed and the majority of the cases are sporadic in occurrence. The clinical phenotype of GS is highly variable and multiple associated anomalies of various organ systems have been reported in the literature. The term “Expanded Goldenhar Complex” has been used when there are associated unusual extrafacial abnormalities involving major organ systems such as the central nervous system, cardiovascular system, and respiratory system. We report a case of Expanded Goldenhar Complex with multiple anomalies, some of which are very rarely reported associations. A 5-year-old boy presented with right-sided hemifacial microsomia, microtia, preauricular and malar skin tags, bilateral radial club hands, and scoliosis since birth. Imaging revealed additional abnormalities including aural atresia, unilateral pulmonary agenesis, dextrocardia, vertebral segmentation defects, left renal ectopia, and right undescended testis. Surgical corrections were undertaken for the right radial club hand and undescended testis and he is awaiting surgery for the left club hand. Complete imaging evaluation of children with dysmorphic facies and limb abnormalities helps in identifying the various associated organ anomalies and to arrive at an accurate syndromic diagnosis. These patients have to be managed by a multidisciplinary team of clinicians on a case-to-case basis and have a good prognosis if there are no major cardiac defects or intellectual disability.
Keywords
Expanded Goldenhar Complex
Pulmonary agenesis
Radial club hands
Oculoauriculovertebral spectrum
Hemifacial microsomia

INTRODUCTION
Goldenhar syndrome (GS) also known by the term first and second branchial arch syndrome, belonging to the facioauriculovertebral (FAV) spectrum or oculoauriculovertebral (OAV) spectrum, is a disorder of craniofacial morphogenesis primarily involving the structures derived from the first and second pharyngeal arches, intervening first pharyngeal pouch and branchial cleft.[1-4] The reported prevalence of the entire OAV spectrum (OAVS) is approximately 3.8/100,000 live births.[1] Here, we report a case of a 5-year-old boy with craniofacial dysmorphism associated with multiple extrafacial anomalies such as bilateral club hands, right lung agenesis, dextrocardia, renal ectopia, and undescended testis conforming to the syndromic diagnosis of Expanded Goldenhar Complex. Emphasis is given to the role of imaging and the differentials to be considered in the evaluation of patients with facial dysmorphism and anomalies affecting multiple organ systems.
CASE REPORT
A 5-year-old boy of normal intellectual development having dysmorphic facies, with deformities of both hands and limitation of hand movements since birth was brought to the orthopedics outpatient department. There was no history of similar deformities in the family or parental consanguinity. There was a history of 5-day neonatal intensive care unit stay for respiratory distress in the postnatal period. On examination, the child had right-sided plagiocephaly, hemifacial microsomia, microtia, preauricular and malar skin tags, short neck with mild torticollis, and scoliosis, apart from bilateral radial club hands [Figure 1]. There was no obvious ocular abnormality and the child had normal vision of both eyes. Given the multiple anomalies, he was investigated with a skeletal survey. Radiographs of bilateral forearms with hands revealed absent right radius and distal phalanx of thumb and syndactyly of the 2nd and 3rd digits of the right hand, hypoplasia of the left radius, posterolateral bowing of the left ulna, elongated 2nd metacarpal, and synpolydactyly of 3rd digit of the left hand [Figure 2]. The radiograph of the skull with cervical spine anteroposterior and lateral views showed subtle hypoplasia of the right-sided facial bones and S-shaped scoliosis of the cervicothoracic spine, associated with segmentation anomalies in the form of butterfly vertebrae of C5, C6, C7, T4, and T7 and hemivertebra in T3. The segmentation anomalies of the cervicothoracic vertebrae were confirmed in computed tomography (CT) thorax [Figure 3].
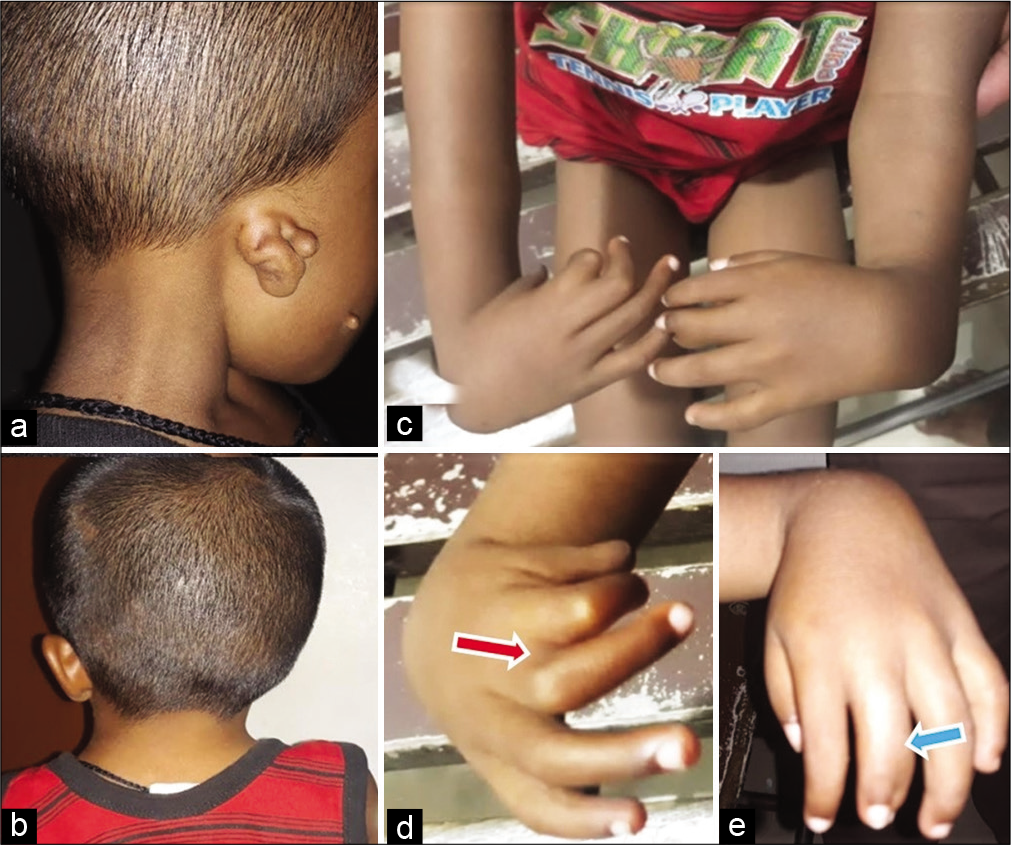
- Photographs showing (a) right microtia Grade II (abnormal auricle without some identifiable landmarks) and preauricular and malar skin tags (b) short neck with and mild torticollis (c) radial club hand deformity of both hands with hands perpendicular to forearms (d) right hand showing hypoplastic thumb and index finger, and partial syndactyly of the 2nd and 3rd digits (red arrow) and (e) left hand showing broadened 3rd digit (blue arrow).
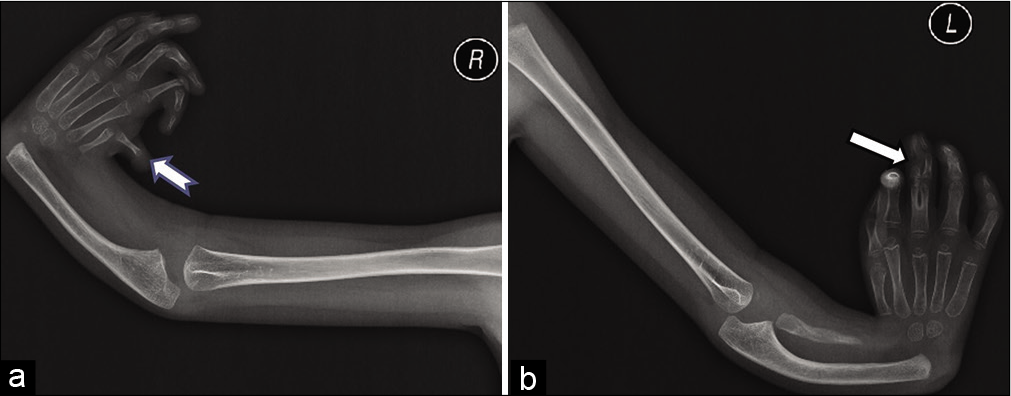
- (a) Anteroposterior (AP) radiograph of the right upper limb showing absent radius and distal phalanx of thumb (notched arrow), radial deviation of hand with a perpendicular orientation of hand with respect to the forearm, and delayed ossification of carpal bones. (b) AP radiograph of the left upper limb showing hypoplastic radius, bowing of ulna, radial deviation of hand with a perpendicular orientation of hand with respect to the forearm, delayed ossification of carpal bones, elongated 2nd metacarpal, and synpolydactyly of 3rd digit (solid arrow).
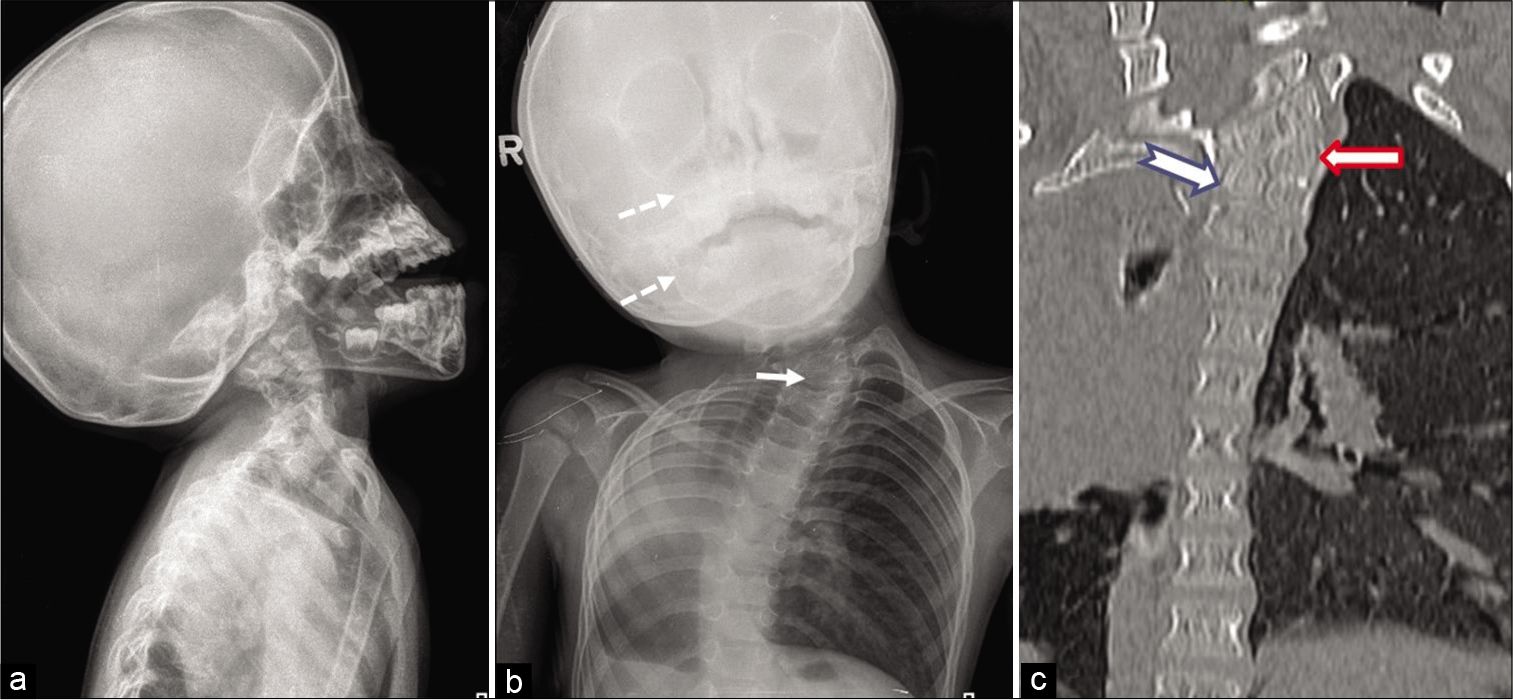
- Radiographs of the skull with cervical spine (a) anteroposterior view and (b) lateral view showing asymmetry of facial bones (maxillary sinus and mandible – dotted arrows), S-shaped scoliosis of the cervicothoracic spine and hemivertebra of T3 (arrow) (c) coronal multiplanar reconstruction image of the cervicothoracic spine showing T3 hemivertebra (solid arrow) and T4 butterfly vertebra (notched arrow).
Chest X-ray posteroanterior view showed a shift of the heart and mediastinum to the right hemithorax and hyperlucency in the right mid and lower lung zones [Figure 4a]. Echocardiography confirmed the dextroversion of the heart without any other structural anomaly. High-resolution CT (HRCT) of the thorax showed blind-ending right main bronchus with absent right lung parenchyma suggestive of agenesis. Besides, there was compensatory hyperinflation of the left lung herniating to the right hemithorax explaining the radiolucency in the chest radiograph [Figure 4b-d]. HRCT of temporal bone showed the absence of external auditory canal, dysplastic middle ear cavity, severely narrowed internal acoustic canal, and non-pneumatization of mastoid air cells on the right side [Figure 5]. Ultrasonography (USG) of the abdomen revealed an ectopic malrotated left kidney on the left side of the pelvis and undescended right testis in the right inguinal canal. These multiple abnormalities prompted us to look for a syndrome into which all these features would fit in. An extensive search of literature led us to the final diagnosis of “Expanded Goldenhar Complex.” The child was referred to the plastic surgery department for the correction of the deformities of hands and underwent soft-tissue release and centralization of the right hand [Figure 6]. Eight months later, he also underwent laparoscopic orchidopexy for the right undescended testis in the department of pediatric surgery. At present, he is under follow-up and awaiting corrective surgery for the left club hand.
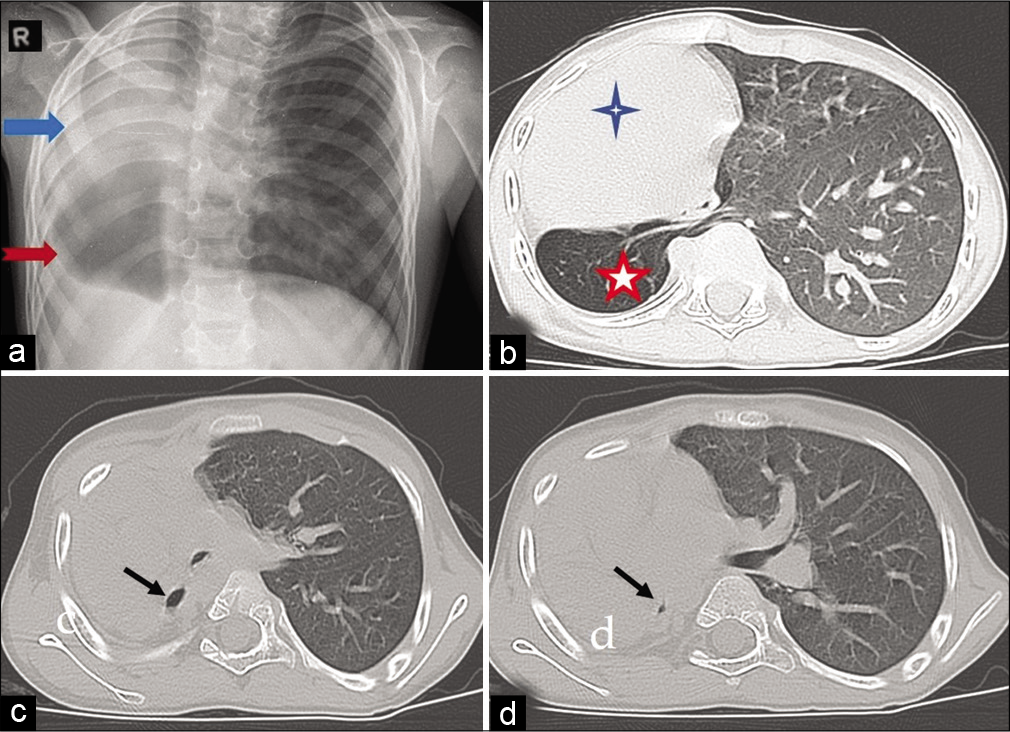
- (a) Chest X-ray anteroposterior view showing a shift of heart and mediastinum to the right hemithorax (blue solid arrow), and radiolucency in the right mid and lower zones (red notched arrow). (b-d) High-resolution computed tomography scan of thorax showing dextrocardia (blue 4-point star)and herniation of the left lung to the right hemithorax behind heart (red 5-point star), blind-ending right main bronchus, and agenesis of the right lung (black arrows).
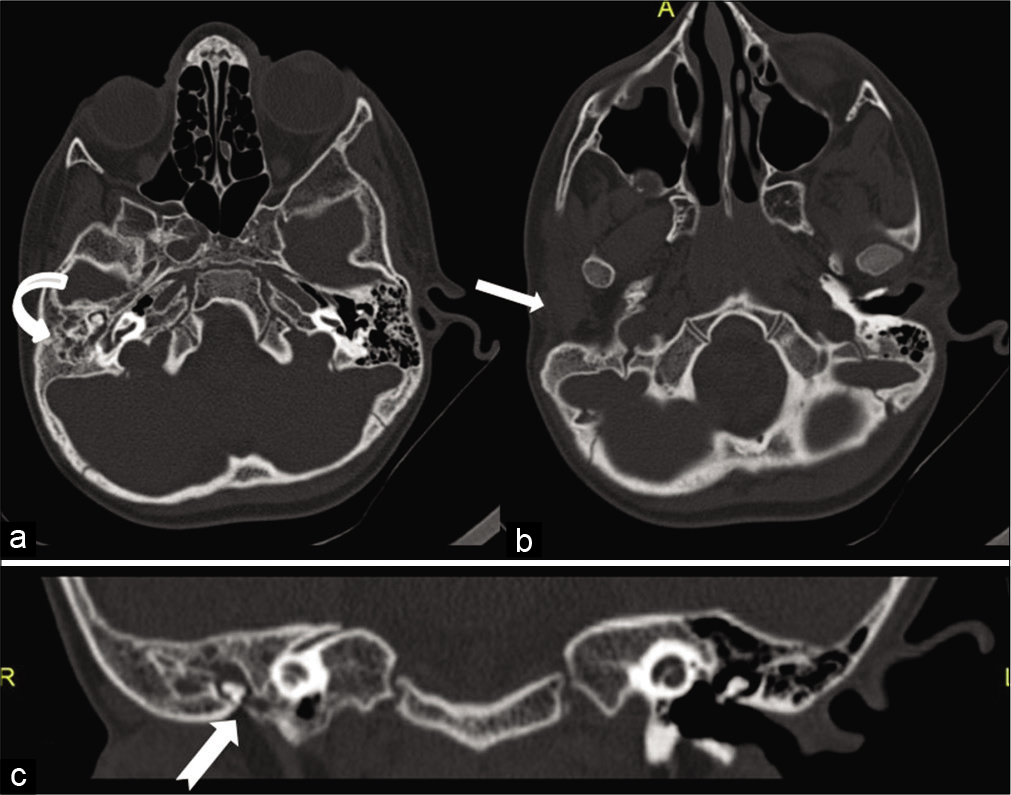
- High-resolution computed tomography of temporal bone axial sections showing (a) dysplastic right middle ear cavity and non-pneumatization of the right mastoid air cells (curved arrow) (b) absent right external auditory canal (solid arrow) (c) coronal reconstructed view showing small tympanic cavity with dysplastic ossicles (notched arrow).

- X-ray right forearm (a) anteroposterior and (b) lateral views post-centralization procedure showing K-wire in situ passed through the 4th metacarpal to restore carpus in line with the ulna.
DISCUSSION
Franceschetti-GS, or Goldenhar-Gorlin syndrome, also known as FAV spectrum, first and second branchial arch syndrome, or OAVS is a disorder of craniofacial morphogenesis primarily involving the structures derived from the first and second pharyngeal arches intervening first pharyngeal pouch and branchial cleft.[5] The prevalence of OAVS ranges from 1/3500 to 1/45,000 according to various authors and the most frequently cited prevalence is 1/3500– 5600 births with a slight male preponderance, male-to-female ratio being 3:2.[1-4] Barisic et al. reported the prevalence of this condition as 3.8/100,000 births (1/26,370) based on the data from EUROCAT, a large network of population-based congenital anomaly registries in Europe. This syndrome was initially observed by Canton in 1861 and later by Carl Ferdinand Von Arlt in 1881. Maurice Goldenhar, an ophthalmologist in 1952, described the syndrome in detail and thus it came to be known as GS. Gorlin et al. in 1963 suggested the name OAV dysplasia to include vertebral anomalies.[6,7]
GS is usually sporadic, however, there have been reports of genetic transmission in literature with autosomal dominant, or, less frequently, autosomal recessive inheritance. A multifactorial etiology including chromosome abnormalities, single gene mutation, vascular disruption, and teratogens (thalidomide, retinoic acid, vasoactive drugs, etc.), maternal infection with rubella and influenza, maternal diabetes, maternal smoking, and multifetal pregnancy has been proposed, affecting the embryological development of the first and second branchial arches and vertebral elements during 3–5 weeks of embryonic life. There are variable expressivity and wide range of phenotypes in GS. A typical phenotype includes microtia, facial asymmetry, and epibulbar dermoids and the minimum criterion accepted for diagnosis is (1) hemifacial microsomia with preauricular tags or (2) microtia with or without preauricular skin tags. Multiple abnormalities involving various organ systems are reported to be associated with GS [Table 1].[4,5,8]
| Head, neck, and face | Hemifacial microsomia, short neck, torticollis, webbed neck, macrocephaly, microcephaly, macrostomia or facial cleft, facial nerve palsy, mandibular hypoplasia, malformed glenoid fossa, velopharyngeal insufficiency, branchial fistula |
|---|---|
| Auricular | Preauricular tags and sinuses, dysplastic ear, microtia, anotia, conductive hearing loss |
| Ocular | Epibulbar dermoid, upper eyelid coloboma, microphthalmia, orbital dystopia, lacrimal duct atresia, or stenosis |
| Cardiac | Tetralogy of Fallot, transposition of great vessels, septal defects, dextrocardia, situs inversus, aortic stenosis, pulmonary artery anomalies |
| Respiratory | Pulmonary agenesis or hypoplasia |
| Gastrointestinal | Tracheoesophageal fistula, atresia, anal anomalies |
| Renal | Renal ectopia, unilateral renal agenesis, double ureter, hydronephrosis |
| Central nervous system | Microcephaly, encephalocele, corpus callosum agenesis, Arnold Chiari malformation, holoprosencephaly |
| Skeletal | Radial limb anomalies, polydactyly, syndactyly, clinodactyly, clubbing of fingers and toes, rocker bottom feet, abnormal foot position Vertebral anomalies – hemivertebrae, cervical fusion abnormalities, basilar invagination, scoliosis, Sprengel deformity Frontal plagiocephaly |
| Genital | Undescended testis, absent hymen, hypospadias |
| Abdominal wall | Umbilical hernia, inguinal hernia, diastasis recti |
Although there are no established diagnostic criteria for the term “Expanded Goldenhar Complex,” it is used when GS is associated with uncommon extrafacial but clinically remarkable anomalies such as those of the central nervous system, cardiovascular system, and respiratory system.[2,4] Our case had the classical craniofacial anomalies of GS such as hemifacial microsomia, microtia, aural atresia, preauricular, and malar skin tags all on the right side, associated with vertebral anomalies. Besides, he also had significant extrafacial anomalies such as bilateral radial club hands, right pulmonary agenesis, dextrocardia, ectopic left kidney, and undescended right testis, and hence, the case is categorized as an Expanded Goldenhar Complex. According to the review article by Heike et al., mandibular hypoplasia and microtia are the most frequent craniofacial anomalies with a prevalence of 44–100% and 66–99%, respectively, and 65% of individuals with GS will have some degree of facial asymmetry. Abnormalities are unilateral in 85% of cases and bilateral in 10–33% with the right side more frequently affected.[6,8,9] In our case also, the right side was more severely affected. There were no ocular manifestations in our case which has a reported prevalence of 4–35%.[8] Cardiac anomalies are reported in approximately 4–33% and the most commonly reported cardiac anomalies are Tetralogy of Fallot and septal defects, whereas dextrocardia is a comparatively rarer occurrence. Among the genitourinary anomalies, cryptorchidism is reported but rare. Pulmonary anomalies are the least common among the associated anomalies with a prevalence of 1–15%.[8]
The diagnosis of GS is clinical and radiological. Karyotyping and genetic analysis may help only in a small percentage of cases as the majority are sporadic. While considering the differential diagnosis for our case, various syndromes with similar types of multiorgan involvement were considered. A close differential is Nager acrofacial dysostosis which is a combination of mandibulofacial dysostosis with radial hypoplasia or triphalangeal thumb with or without temporomandibular joint ankylosis, ear anomalies, ocular abnormalities, genitourinary anomalies, and congenital cardiac anomalies.[8] Our patient had hemifacial microsomia rather than microretrognathia which made it more likely to be GS than Nager syndrome, though the rest of the features are overlapping in both.
Another diagnosis to be considered with this combination of anomalies is VACTERL association which refers to a combination of vertebral anomalies, anal atresia, cardiac defects, tracheoesophageal – fistula/Esophageal atresia, renal defects, and limbs defects.[8,10] The presence of craniofacial dysmorphism and pulmonary agenesis and the absence of anal and tracheoesophageal anomalies were against the VACTERL association in our case though the rest of the findings can be considered as conforming to this entity.
The treatment of OAVS is tailored according to the age, symptoms, deformities, and disabilities of the individual patient. Multidisciplinary teamwork will be needed for the management, especially in cases with the involvement of multiple organ systems. Prognosis is generally good in the absence of mental retardation and major cardiac anomalies.[5,8]
In our case, various imaging modalities such as X-ray, CT, echocardiography, and USG were done to assess the involvement of various organs. Deformity due to the radial club hand of the right side was managed by plastic surgeons who did soft-tissue release and centralization. Cryptorchidism was managed with orchidopexy by the pediatric surgeon.
CONCLUSION
GS is the most severe form of OAV spectrum, and the term Expanded Goldenhar Complex is to be used when there are associated unusual extrafacial anomalies. The diagnosis of these syndromes is by detailed clinical examination supported by the skeletal survey, USG abdomen, and echocardiography and resorting to other modalities such as CT and magnetic resonance imaging on a case-to-case basis depending on the systems involved. Since many of these syndromes have a sporadic etiology rather than genetic, a confirmation will most likely depend on the imaging features. A combination of craniofacial dysmorphism, radial deficiencies, and vertebral segmentation anomalies, with the involvement of pulmonary, cardiac, or genitourinary systems should raise the possibility of Expanded Goldenhar Complex among the various close differentials.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Prevalence, prenatal diagnosis and clinical features of oculo-auriculo-vertebral spectrum: A registry-based study in Europe. Eur J Hum Genet. 2014;22:1026-33.
- [CrossRef] [PubMed] [Google Scholar]
- Caudal regression and encephalocele: Rare manifestations of expanded goldenhar complex. Case Rep Pediatr. 2017;2017:4396142.
- [CrossRef] [PubMed] [Google Scholar]
- Oculo-auriculo-vertebral spectrum: Clinical and molecular analysis of 51 patients. Eur J Med Genet. 2015;58:455-65.
- [CrossRef] [PubMed] [Google Scholar]
- Oculoauriculovertebral dysplasia and variants: Phenotypic characteristics of 294 patients. Am J Med Genet. 1987;26:361-75.
- [CrossRef] [PubMed] [Google Scholar]
- Oculo-auriculo-vertebral spectrum: A review of the literature and genetic update. J Med Genet. 2014;51:635-45.
- [CrossRef] [PubMed] [Google Scholar]
- Craniofacial microsomia overview-archived chapter, for historical reference only In: Adam MP, Ardinger HH, Pagon RA, Wallace SE, Bean LJ, Stephens K, eds. Gene Reviews®. Seattle, WA: University of Washington; 1993.
- [Google Scholar]
- Oculoauriculovertebral spectrum: An updated critique. Cleft Palate J. 1989;26:276-86.
- [Google Scholar]
- Goldenhar syndrome: Clinical features with orofacial emphasis. J Appl Oral Sci. 2010;18:646-9.
- [CrossRef] [PubMed] [Google Scholar]




