
Translate this page into:
Intraosseous schwannoma of inferior pubic ramus – A rare benign osseous neoplasm

*Corresponding author: Ramakrishna Narayanan, Department of Radiology. Nizam’s Insitute of Medical Sciences Panjagutta, Hyderabad, Telanagana, India. drrkris@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Lamani PU, Narayanan R, Rakesh UN, Rao NK. Intraosseous schwannoma of inferior pubic ramus – A rare benign osseous neoplasm. Indian J Musculoskelet Radiol 2021;3:140-3.
Abstract
Intraosseous schwannomas are a very rare subgroup of schwannomas. They account for <1% of all primary bone neoplasms. The mandible is the most commonly involved bone followed by the sacrum. We herein report a case of intraosseous schwannoma involving the inferior ramus and body of the pubic bone in a 43-year-old male who presented with a swelling in the right groin. On radiographs and computed tomography, it appeared as a mildly expansile, lytic, multiloculated lesion in the right pubic bone with a narrow zone of transition, sclerotic margins with areas of cortical breach, and a significant intra and extrapelvic soft-tissue component which did not show any areas of calcification. On magnetic resonance imaging, it appeared isointense to skeletal muscle on T1-weighted images, mildly hyperintense on T2-weighted images, and markedly hyperintense on short-tau inversion recovery images. The differentials considered on imaging were chondroid neoplasms such as chondromyxoid fibroma or low-grade chondrosarcoma, giant cell tumor, and plasmacytoma. However, biopsy and histopathology revealed an intraosseous schwannoma. The patient was operated and the lesion was excised in toto. Intraoperatively, the origin of the lesion was identified as the right obturator nerve. Post-operative, the patient recovery was uneventful and he was discharged.
Keywords
Intraosseous
Schwannoma
Pubic bone
Lytic lesion
Trucut biopsy

INTRODUCTION
Schwannoma (neurilemmoma) is a benign, slow-growing tumor that arises from the Schwann cells which encase the myelinated nerve fibers forming the neural sheath. It was first described by Verocay in 1910 as a pathological entity.[1,2] Schwannoma is a fairly common soft-tissue tumor and comprises about 5% of all benign soft-tissue tumors.[2] It commonly occurs in the head-and-neck regions, posterior mediastinum, and along the flexor surfaces of extremities.[1,3].Intraosseous schwannoma is rare, accounting for <1% of benign bone tumors, with about 200 cases were described in the worldwide literature.[2-4] It does not show any age or sex predilection.[2] The mandible is the most commonly affected bone, followed by sacrum.[1,2,3,5] To the best of our knowledge, only two cases of intraosseous schwannoma involving iliopubic ramus have been described.[4] Here, we present a rare case of an intraosseous schwannoma of inferior pubic ramus in a middle-aged male.
CASE REPORT
A 43-year-old male presented to the department of orthopedics with complaints of mildly painful swelling on the medial aspect of the right groin for 2 years. The swelling gradually increased in size and was associated with a tingling and dragging sensation in the right lower limb. There were no aggravating or relieving factors for the pain. There was no history of fever and constitutional symptoms such as loss of appetite or loss of weight.
On examination, an ill-defined, approximately 8.0 × 8.0 cm swelling was seen in the right pubic region. It was firm, immobile, painless, non-fluctuant, and non-translucent. There was no cough impulse. The skin over the swelling appeared normal but stretched. Blood investigations and inflammatory parameters were unremarkable.
The patient underwent a radiograph of the pelvis [Figure 1] which showed a geographic, mildly expansile, lytic lesion in the right pubic bone involving the body and inferior pubic ramus. It had a narrow zone of transition with sclerotic margins and the matrix showed multiple thick internal trabeculae, giving a “soap bubble” appearance. There were areas of cortical break with associated soft-tissue component, which did not show any areas of calcification or air lucencies within. Ipsilateral obturator foramen was widened and there was scalloping of the medial aspect of the right superior pubic ramus. The patient then underwent a non-contrast computed tomography of pelvis [Figure 2] which confirmed the findings on the radiographs. The soft-tissue component of the lesion was hypodense with a larger extrapelvic and smaller intrapelvic component. The intrapelvic component was extending inferomedially into the ischiorectal and ischioanal fossa with maintained fat planes with the anal sphincters.
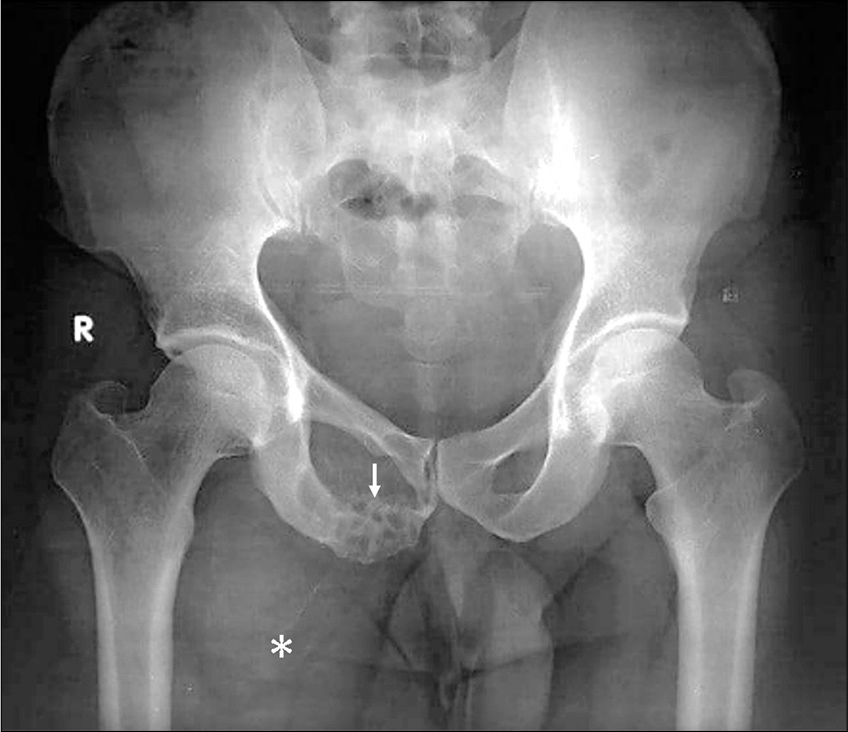
- A 43-year-old man with intraosseous schwannoma of the right inferior pubic ramus who presented with swelling in the right groin. Radiograph of pelvis shows a geographic, mildly expansile lytic lesion in the right pubic bone involving the body and inferior pubic ramus (white arrow) with a narrow zone of transition and thick internal trabeculations, giving a “soap bubble” appearance. There are areas of cortical break with associated soft-tissue component (white asterisk), which did not show any areas of calcification or air lucencies within. Ipsilateral obturator foramen is widened and there was scalloping of the medial aspect of the right superior pubic ramus.
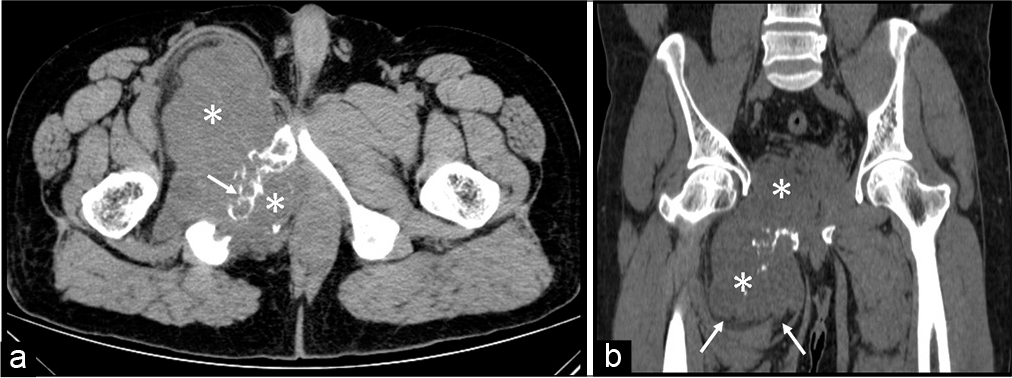
- A 43-year-old man with intraosseous schwannoma of the right inferior pubic ramus who presented with swelling in the right groin. (a) Non-contrast CT axial image shows a geographic, mildly expansile lytic lesion in the right pubic bone involving the body and inferior pubic ramus with a narrow zone of transition and thick internal bony trabeculations (white arrow), giving a “soap bubble” appearance. Areas of cortical break with associated intra and extrapelvic hypodense soft-tissue component (white asterisks) which did not show any areas of calcification within. The intrapelvic component was extending inferomedially into the ischiorectal and ischioanal fossa with maintained fat planes with the anal sphincter. (b) Non-contrast CT coronal image shows that the soft-tissue component (white asterisks) is compressing and displacing the muscles of the thigh with well-maintained fat planes (white arrows).
The extrapelvic component was extending anterolaterally, compressing, and displacing the medial compartment muscles of the thigh with well-maintained fat planes. For further characterization of the lesion, a magnetic resonance imaging (MRI) of pelvis was performed [Figure 3], which showed a large 15.0 × 7.0 × 14.0 cm (CC × TR × AP), well-defined lobulated multiseptate lesion arising from right inferior pubic ramus with intra and extrapelvic components, which was isointense to skeletal muscle on T1-weighted images, mildly hyperintense on T2-weighted images, and markedly hyperintense on short-tau inversion recovery (STIR) images [Figure 2]. The intrapelvic component was compressing the right levator ani muscle and slightly displacing the anal canal to the left, while the large extrapelvic component was seen severely compressing and displacing the pectineus and adductor muscles with maintained fat planes.
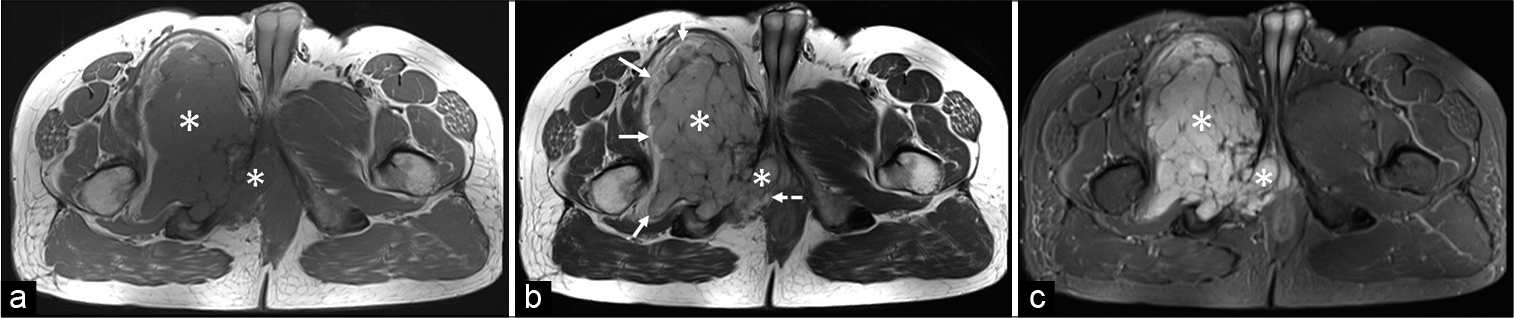
- A 43-year-old man with intraosseous schwannoma of the right inferior pubic ramus who presented with a swelling in the right groin. (a) Non-contrast MRI axial T1-weighted image shows an altered signal intensity lesion in the right pubic bone involving the body and inferior pubic ramus with a narrow zone of transition and a large intra and extrapelvic soft-tissue component (white asterisks) which is isointense to the skeletal muscle. (b) Non-contrast MRI axial T2-weighted image shows the soft tissue (white asterisks) is mildly hyperintense to the skeletal muscle. The soft-tissue component is compressing and displacing the muscles of the thigh with well-maintained fat planes (white arrows). The intrapelvic component shows maintained fat planes with the anal sphincter (dashed white arrow). (c) Non-contrast MRI axial short-tau inversion recovery image shows the soft tissue (white asterisks) is markedly hyperintense to the skeletal muscle.
Based on the clinical and radiological features, the differentials considered were chondroid neoplasms such as chondromyxoid fibroma or low-grade chondrosarcoma (in view of hyperintensity on T2-weighted and STIR images), giant cell tumor, and plasmacytoma.
Ultrasound-guided trucut biopsy was performed using BARD Max-Core disposable core 18 G biopsy gun from the extrapelvic soft-tissue component.
Histopathology [Figure 4] showed multiple Verocay bodies characterized by palisade arrangement of bland spindle cells with oval to elongated nuclei with tapered ends. The intervening areas showed loosely arranged bland spindle cells representing Antoni B areas. There was no significant mitotic activity or any evidence of necrosis. On immunohistochemistry (IHC) with S100 and SOX10, spindle cells showed diffuse strong combined cytoplasmic and nuclear positivity with former and only nuclear staining in the latter. Epithelial membrane antigen and synaptophysin were negative. Based on the above described morphological and IHC findings the final histopathological diagnosis of benign nerve sheath tumor (Schwannoma) was given.
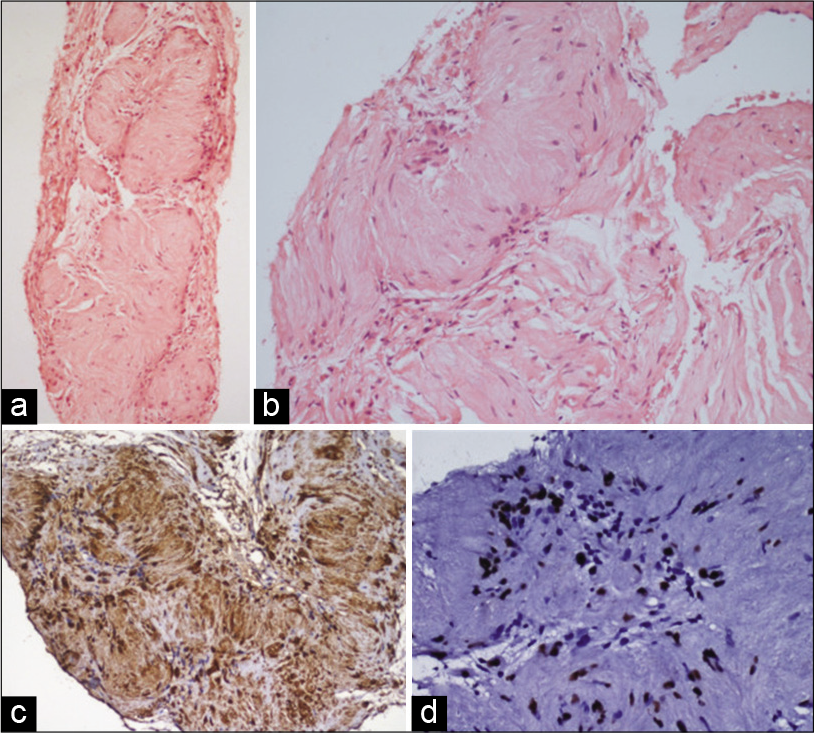
- A 43-year-old man with intraosseous schwannoma of the right inferior pubic ramus who presented with a swelling in the right groin. Histopathology sections show (a) and (b) sections of core biopsy showing multiple Verocay bodies characterized by palisaded arrangement of bland spindle cells representing Antoni A areas. Cells represent Antoni B areas (H&E; a×40, b×200). (c) IHC with S100 showing diffuse strong nuclear and cytoplasmic positivity in spindle cells and (d) IHC with SOX10 showing strong nuclear positivity in the spindle cells (poly HRP; c×200, d×400).
The patient underwent complete en bloc resection of the tumor with Type III pelvic resection surgery. Intraoperative findings showed a well-encapsulated tumor involving the right inferior pubic ramus with maintained fat planes with adjacent structures. The origin of the lesion was noted from the right obturator nerve, which had to be sacrificed [Figure 5]. Gross specimen of the tumor weighed 2.5 kg [Figure 5]. Histological findings of resected specimen were also consistent with diagnosis of schwannoma. Post-surgery, the patient recovery was uneventful and he was discharged with follow-up advice.
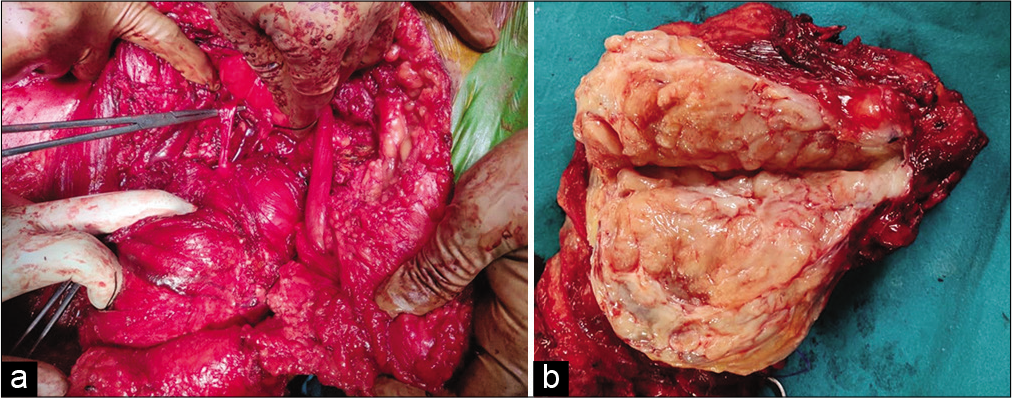
- A 43-year-old man with intraosseous schwannoma of the right inferior pubic ramus who presented with a swelling in the right groin. (a) Intraoperative photograph shows the continuity of the lesion with the right obturator nerve (tip of artery forceps). (b) Photograph of cut section of gross specimen shows tan white material which was gritty and fibrous in nature.
DISCUSSION
Schwannoma also known as neurilemmoma is a benign slow-growing tumor arising from the Schwann cells, which form the sheath of a myelinated nerve fiber.[3,4] They show a predilection for sensory nerves, as these nerve contain more Schwann cells along their axons.[4,6] It is a fairly common soft-tissue tumor, comprising about 5% of all benign soft-tissue tumors.
Intraosseous schwannomas, however, are rare, and this may due to the paucity of sensory nerve fibers in the bone.[4,7] Mandible is the most commonly affected bone, this has been attributed to the long intraosseous course of the mandibular nerve, which is predominantly a sensory nerve.[4,6,8] Other reported locations include long bones of upper and lower limbs, vertebrae, and flat bones such as calvarium, sternum, scapula, ribs, ilium, and patella.[8]
Three mechanisms have been proposed for the involvement of bone by schwannoma. First, they may arise from an intraosseous sensory nerve in the medullary cavity, second, arising in the nutrient canal with a dumbbell configuration, and third, an extraosseous lesion causing secondary erosion and penetration into the bone.[1,3,5] In our case, the third mechanism was probably the process by which the schwannoma arising from the right obturator nerve involved the pubic bone.
The symptoms of schwannomas are often non-specific and depend on the location and extension. Swelling is the most common symptom followed by pain or paresthesia.[1,9]
Imaging findings of intraosseous schwannomas are usually non-specific. On radiographs and CT, they may appear as a well-defined lytic lesion with sclerotic margins, with cortical expansion, cortical erosions, intralesional trabeculations, and absent matrix calcification.[2,5,7,8] Similar findings were seen in our case with a lytic lesion showing sclerotic margins, internal trabeculations, and soft tissue not showing any calcification. These findings, however, are non-specific and may be seen in several other benign bony lesions including aneurysmal bone cyst, giant cell tumor, fibrous dysplasia, desmoplastic fibroma, benign fibrous histiocytoma, chondromyxoid fibroma, and in a few malignant lesions like low-grade chondrosarcoma.[2]
On MRI, schwannomas are solid appearing lesions which are isointense to skeletal muscles on T1-weighted images and heterogeneously hyperintense on T2-weighted and STIR images. Contrast-enhanced sequence may show mild-to-moderate enhancement. MRI demonstrates the soft-tissue extensions and relations to adjacent organs well.[5,7,8] The imaging appearance was similar in our case and MRI demonstrated the well-demarcated tumor margins in great detail, allowing the operating surgeon to use blunt dissection to separate the tumor from its bed.
Schwannomas show poor response to radiotherapy. However, since they are well-encapsulated lesions, surgical enucleation remains the treatment of choice with periodic follow-up.[1]
To the best of our knowledge, this is only the third reported case of intraosseous schwannoma involving the pubic bone. The imaging findings were non-specific and final diagnosis was made only following histological examination of the tissue obtained after biopsy.
CONCLUSION
Intraosseous schwannomas is a very rare benign bony lesion with non-specific imaging features which makes it very difficult to differentiate it from other bony lesions. Radiologists should be aware of this uncommon tumor and consider it among the differentials when imaging findings demonstrate a well-defined, osteolytic lesion with matrix or soft tissue not showing calcifications.
Acknowledgment
We express our deepest gratitude to Prof. Shantveer G. Uppin, Professor, Department of Pathology for providing the histopathology images and legends.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Intraosseous schwannoma of the mandible. J Oral Maxillofac Pathol. 2012;16:294-6.
- [CrossRef] [PubMed] [Google Scholar]
- Intraosseous neurilemmoma of the proximal ulna. Int J Surg Case Rep. 2014;5:914-8.
- [CrossRef] [PubMed] [Google Scholar]
- Giant intraosseous schwannoma of scapula: A rare case report and review of the literature. Diagn Pathol. 2014;9:31.
- [CrossRef] [PubMed] [Google Scholar]
- Giant intraosseous schwannoma of the ileopubic ramus. Orthopedics. 2013;36:982-5.
- [CrossRef] [PubMed] [Google Scholar]
- Intraosseous schwannoma: Case report and review of the literature. Rev Bras Ortop (Sao Paulo). 2020;55:258-62.
- [CrossRef] [PubMed] [Google Scholar]
- Intraosseous schwannoma of the calcaneus: A rare tumor of the bone. Case Rep Orthop. 2018;2018:9824025.
- [CrossRef] [PubMed] [Google Scholar]
- Intraosseous schwannoma of the glenoid: Case report and literature review. SICOT J. 2021;7:2.
- [CrossRef] [PubMed] [Google Scholar]
- Intraosseous schwannoma of the ilium. Clin Imaging. 2015;39:161-4.
- [CrossRef] [PubMed] [Google Scholar]
- Solitary intraosseous schwannoma of the base and vault of the skull: A summary review of such unusual location. Clin Sarcoma Res. 2015;5:6.
- [CrossRef] [PubMed] [Google Scholar]




