
Translate this page into:
Magnetic resonance imaging patterns of shoulder injuries in strength trainers

*Corresponding author: Hema Nalini Choudur, Department of Radiology, McMaster University, Hamilton, Ontario, Canada. hnalinic@yahoo.com
-
Received: ,
Accepted: ,
How to cite this article: Ariyanayagam T, Kollimarla VS, Rachakonda A, Choudur HN. Magnetic resonance imaging patterns of shoulder injuries in strength trainers. Indian J Musculoskelet Radiol. 2023;5:162-7. doi: 10.25259/IJMSR_31_2023
Abstract
Weightlifting, a recent addition to strength training regimes of elite athletes, offers various benefits such as increased muscle/tendon/bone strength, bone density, metabolism, and cardiac function. Although beneficial, weightlifting can contribute to various shoulder pathologies that include rotator cuff impingement and injuries to tendons/muscles/bones of the shoulder and shoulder girdle, with specific patterns of injury identified on magnetic resonance imaging (MRI). Our pictorial essay, therefore, aims to familiarize radiologists and sports medicine physicians with the mechanisms, various types, and MRI patterns of shoulder/shoulder-girdle injuries, thereby enabling appropriate alterations to training regimens to prevent further injury.
Keywords
Acromioclavicular joint
Athletes
Glenohumeral joint
Magnetic resonance imaging
Rotator cuff
Shoulder injuries
Strength training
Weightlifting

INTRODUCTION
Strength training through weightlifting exercises (particularly the “clean-and-jerk,” a two-move lift) has increasingly become a prevalent part of athletes’ training regimens.[1-4] The first movement, the “clean,” is the lifting of the barbell from the ground to a resting position on the lifter’s shoulders [Figure 1a]. The second movement is the “jerk” wherein both arms are extended to lift the barbell above the head [Figure 1b].[4] With the clean-and-jerk maneuver, the goal is to develop strength by lifting the maximum weight possible in one repetition.[4] Although weightlifting has many benefits including increased muscle/tendon/bone strength, bone density, metabolism, and cardiac function, it can also lead to injuries, as the body is exposed to great forces.[5-9]
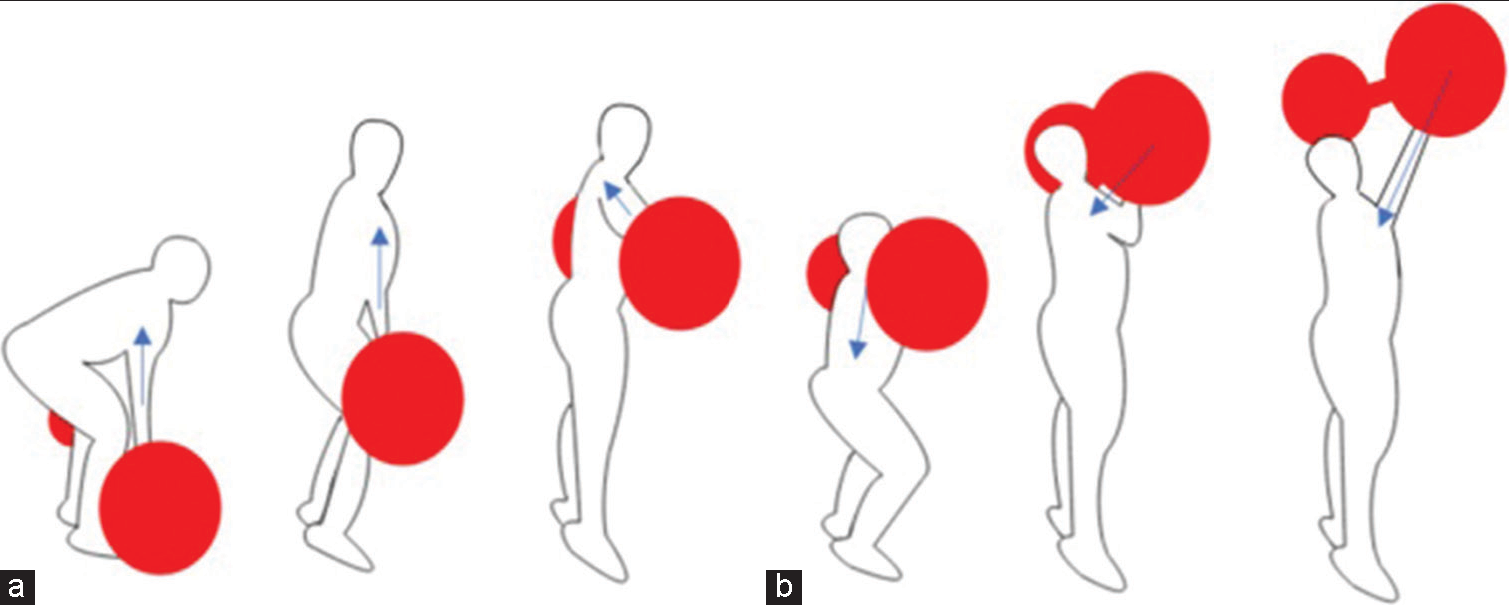
- (a and b) Diagrams depicting the clean-and-jerk phases of weightlifting. The transmission of vector force changes through each phase of this exercise.
Weightlifting most commonly injures the shoulder joint, followed by the lower back and elbow.[10,11] The spectrum of shoulder injuries can be ascribed to the transmission of force through the shoulder girdle during the phases of the clean-and-jerk. At the end of the “clean” phase, the weight is transmitted vertically through the lateral clavicles and acromioclavicular (AC) joints. During the “jerk,” as the weight is lifted to full overhead extension, force is transmitted through the glenohumeral joint and the inferior joint capsule.[4]
In this pictorial assay, we present the commonly seen magnetic resonance imaging (MRI) patterns of shoulder injuries caused by weightlifting regimens of elite athletes referred to the radiology department of our tertiary sports-medicine center. These patients had a history of shoulder pain and/or limited range of movement. The patients did not have any history of direct shoulder injury relating to a contact sport (i.e., football/wrestling/basketball) or other forms of strength training. Specific injury patterns relating to the biomechanics of weightlifting are discussed in this article.
DISCUSSION
By the end of the “clean” phase, the force of the weight is transmitted vertically through the lateral clavicles and AC joints [Figure 2a]. During the “jerk,” the weight is lifted to full overhead extension and the force is transmitted through the glenohumeral joint in a craniocaudal direction along the line of the vector force [Figure 2b].[12,13] The MR images demonstrate that the injuries sustained during these two maneuvers occur exclusively along the line of force.
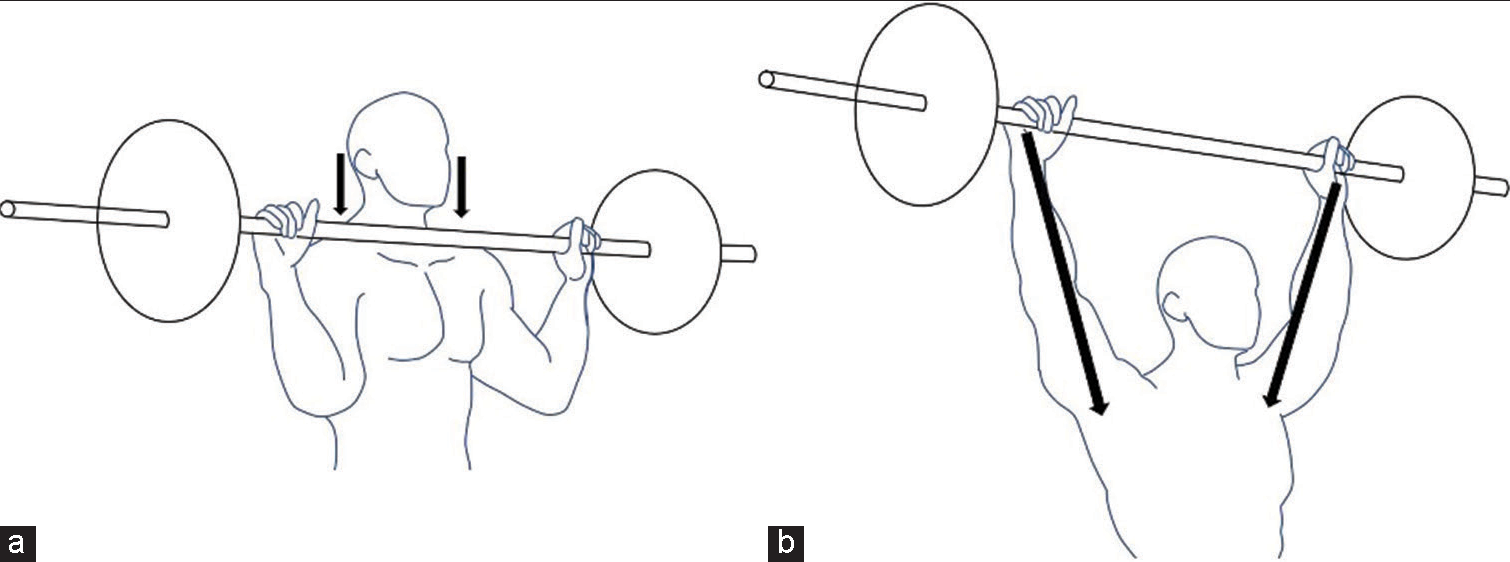
- Diagrams showing (a) the resting phase of the clean and (b) the end of the jerk. After elevating the barbell in the clean phase, the weights rest on the lateral clavicles and acromioclavicular joints (ACJ). The force is transmitted vertically through the lateral clavicle and ACJ (black arrows), resulting in injuries to the clavicle and ACJ/capsule. At the end of the jerk phase, the weights are held at extension over the head. Injury to the deltoid, rotator cuff, glenohumeral ligaments, glenoid labrum, and glenohumeral joint capsule can be attributed to the forces transmitted (black arrows) along the line of the vector force.
The AC joint injuries include AC joint sprain [Figure 3], capsule-ligamentous complex tears [Figure 4], joint separation, and post-traumatic arthropathy [Figure 5]. Tendon injuries include deltoid tendon tears [Figure 6], rotator cuff tendinosis [Figure 7], and rotator cuff tears [Figures 8 and 9]. Rotator cuff pathologies include rotator cuff hypertrophy leading to pseudo-impingement from overfilling of the subacromial space [Figure 10]. Injuries of the glenohumeral joint include labrum [Figure 11], capsule, and glenohumeral ligamentous injuries [Figures 12 and 13]. Bony injuries include distal clavicle [Figure 14] and coracoid [Figure 15] stress reactions, marrow edema, traction edema, and cystic changes at the greater tuberosity of the humerus at the attachment of the rotator cuff tendons [Figure 16].
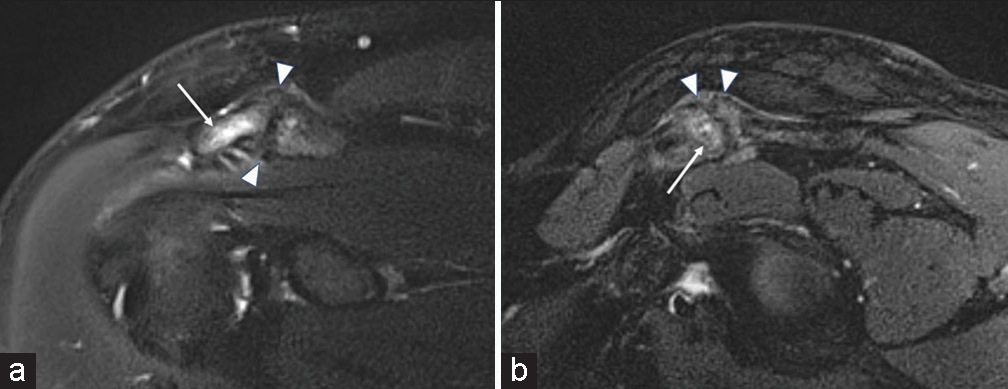
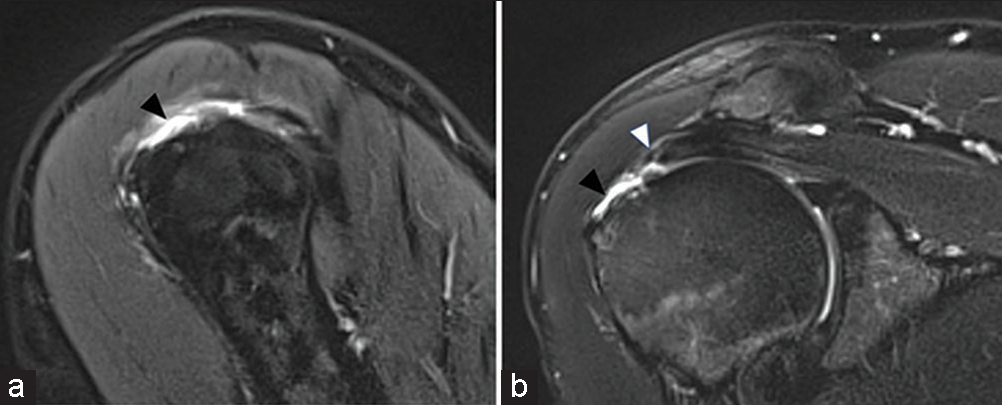
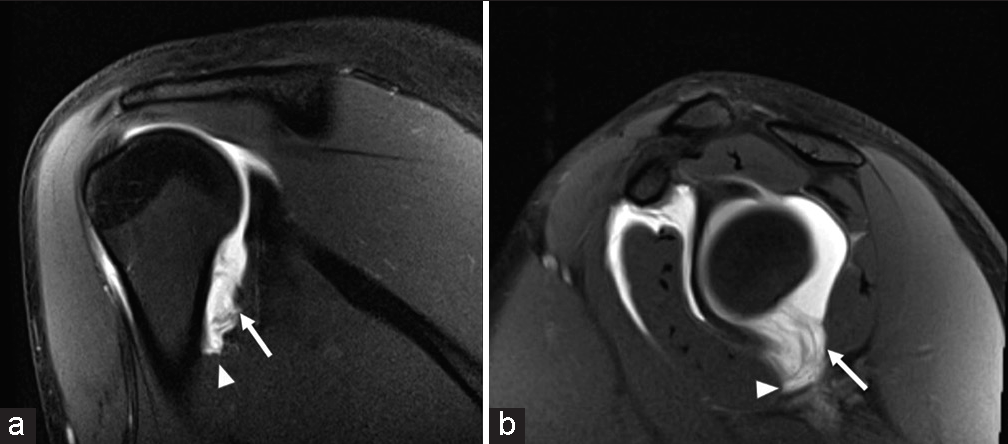
- A 34-year-old male presenting with shoulder pain. T2-weighted fat-saturated (a) coronal and (b) sagittal magnetic resonance images demonstrating acromioclavicular joints sprain. Note bone marrow edema of the acromion (white arrows), thickening of the joint capsule-ligament complex (white arrowheads), and inhomogeneous intact capsule fibers.
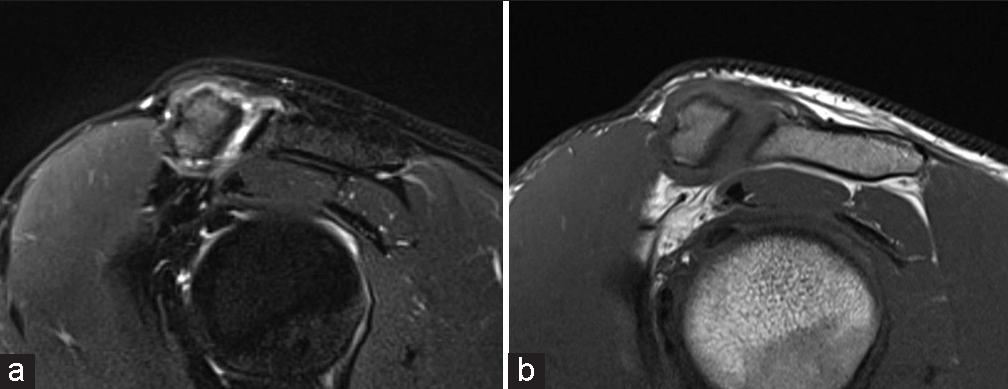
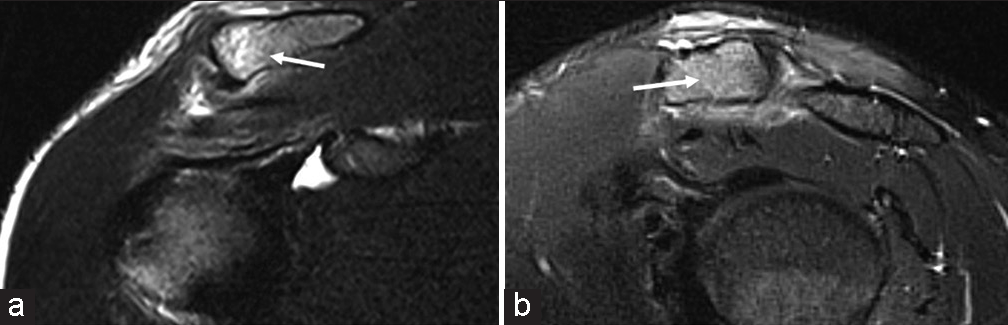
- A 40-year-old male presenting with shoulder pain. (a) T2-weighted fat-saturated and (b) T1-weighted sagittal magnetic resonance images demonstrating acromioclavicular joints (ACJ) capsule rupture. The ACJ capsule-ligament complex is disrupted at the superior joint. A small joint effusion/hemarthrosis is also noted.
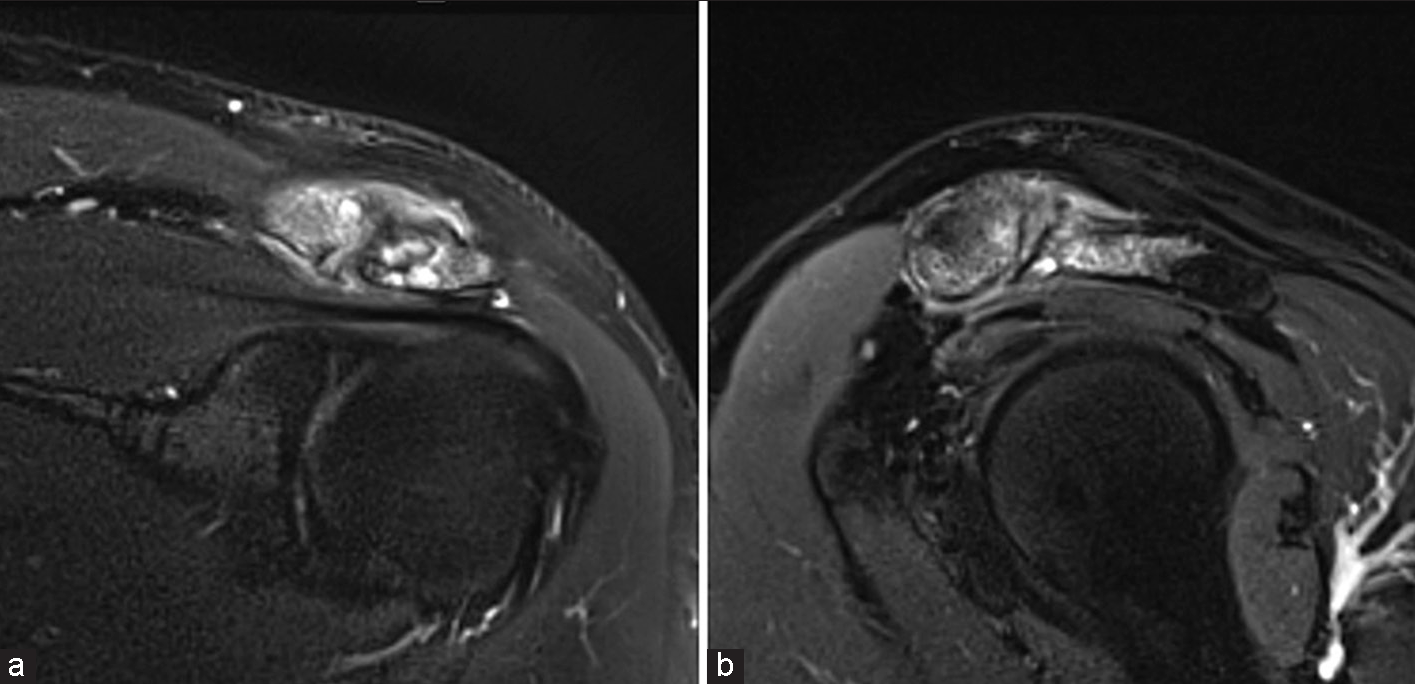
- A 36-year-old male presenting with subacute shoulder pain. T2-weighted fat-saturated (a) coronal and (b) sagittal magnetic resonance images demonstrating post-traumatic acromioclavicular joints (ACJ) arthropathy. Note severe bone marrow edema of the lateral clavicle and acromion, subarticular cysts, and thickening of the ACJ capsule with surrounding soft-tissue edema.
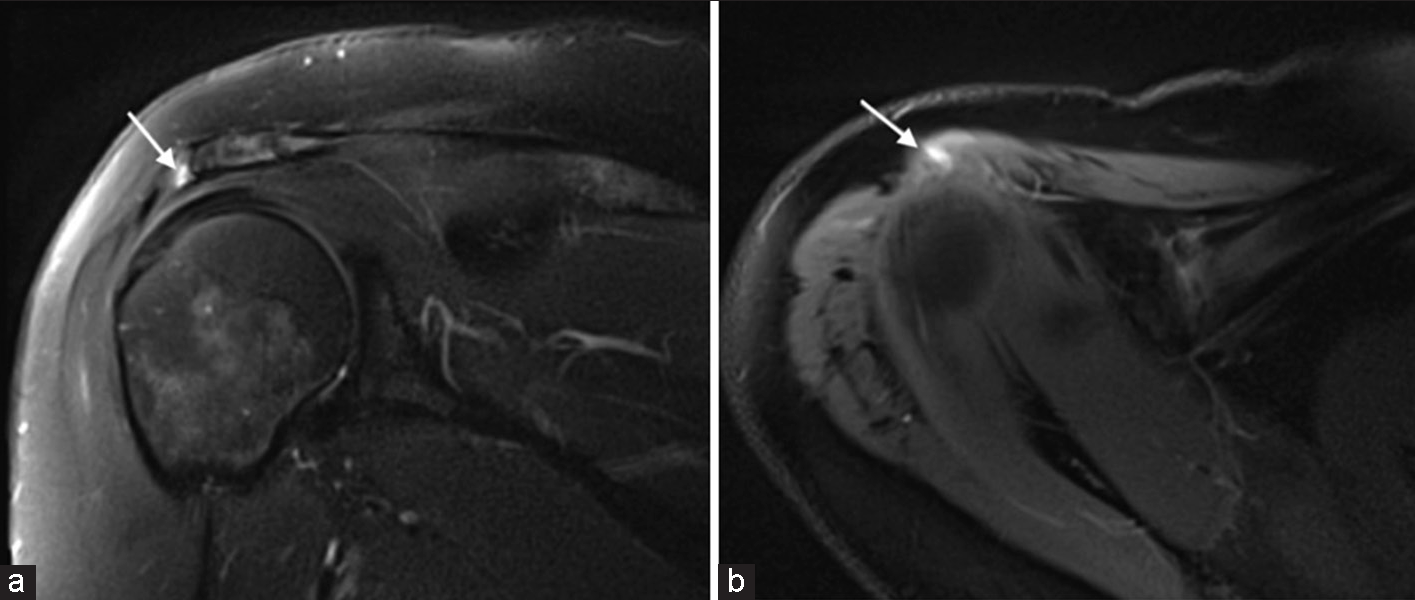
- A 40-year-old female presenting with shoulder pain. T2-weighted fat-saturated (a) coronal and (b) axial magnetic resonance images demonstrating an intrasubstance tear of the acromial attachment of the deltoid tendon. Note linear high signal within the tendon attachment (white arrows).
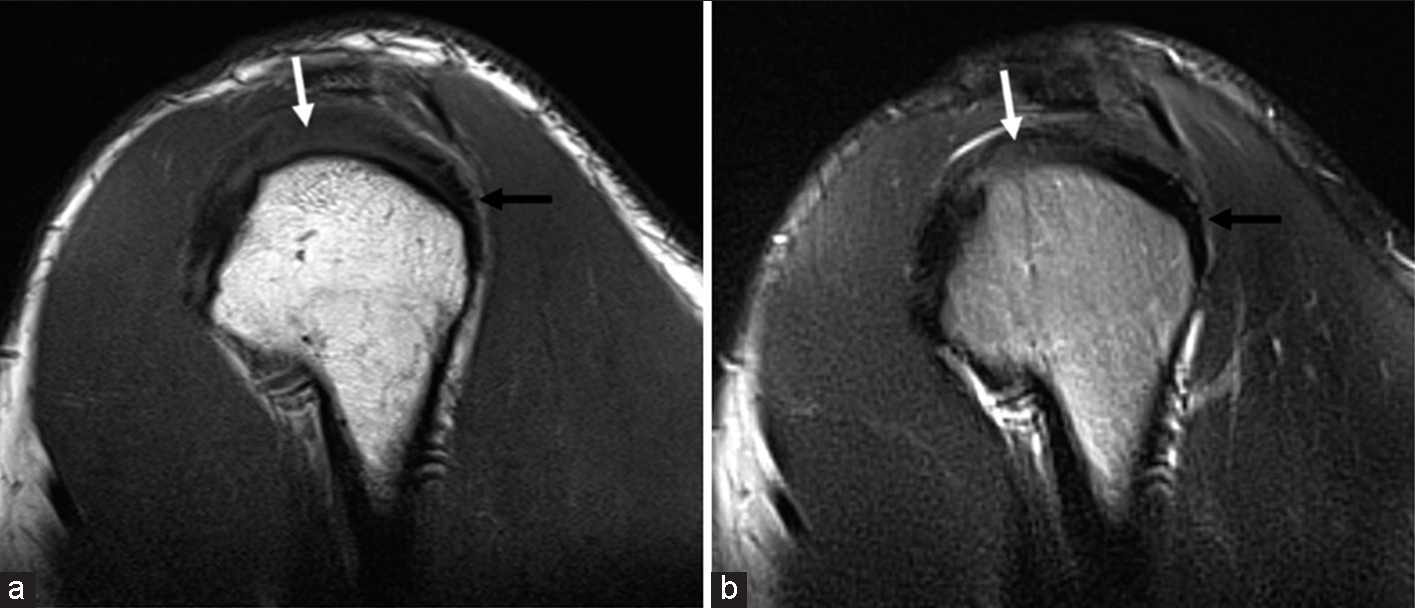
- A 31-year-old male presenting with shoulder pain. (a) T1-weighted sagittal and (b) T2-weighted sagittal magnetic resonance images demonstrating supraspinatus tendinosis with intermediate T1/T2 tendon signal (white arrow). The normal infraspinatus tendon demonstrates dark T1/T2 signal (black arrow).
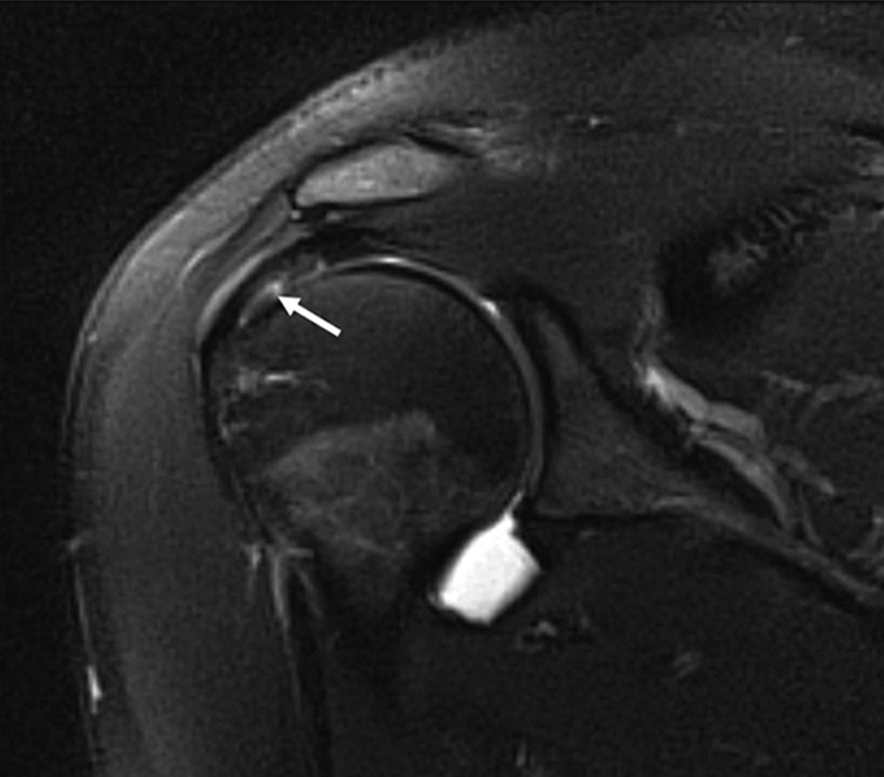
- A 34-year-old female presenting with shoulder pain. T1-weighted fat-saturated coronal magnetic resonance arthrogram demonstrating a partial thickness articular surface tear of the supraspinatus tendon (white arrow).
- (a and b) A 44-year-old male presenting with shoulder pain. T2-weighted fat-saturated coronal magnetic resonance image demonstrating supraspinatus pseudo-impingement (black arrow head). There is hypertrophy of the supraspinatus muscle with increased muscle bulk and paucity of intramuscular fat. Similar changes are seen in the other periarticular muscles. There is overfilling of the subacromial space by the hypertrophied distal muscle belly and myotendon with resultant secondary indentation (white arrow head) of these structures by the overlying acromion and acromioclavicular joint, resulting in clinical features of impingement.
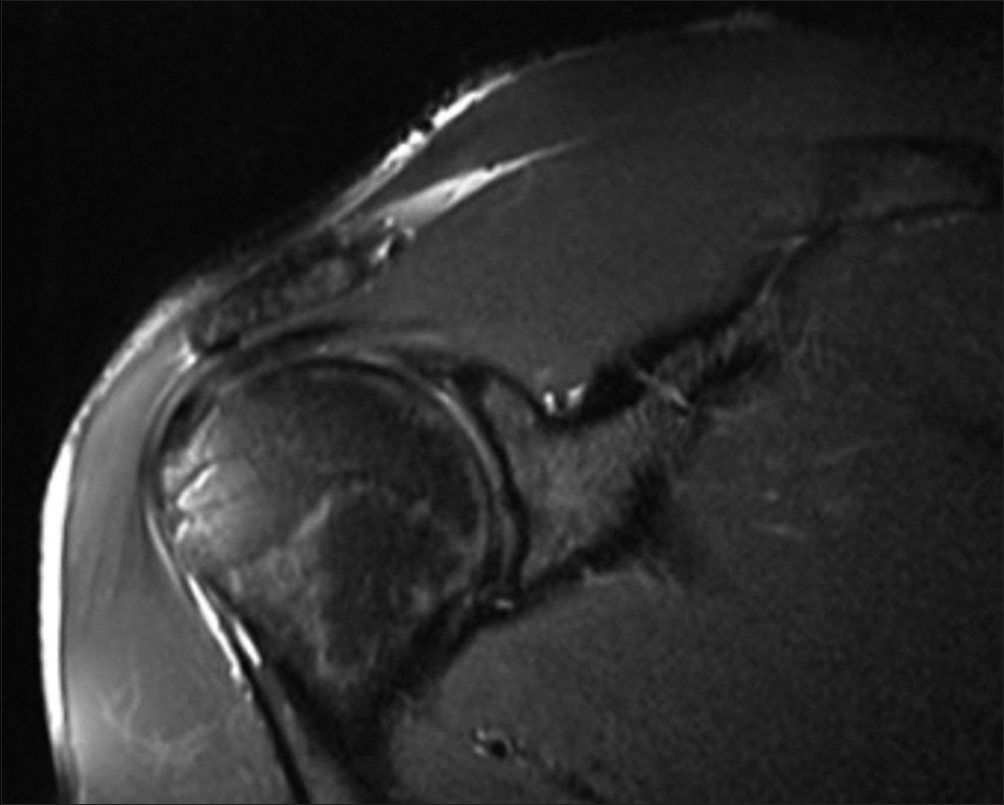
- A 28-year-old male presenting with shoulder pain and decreased range of abduction. T2 weighted fat saturated coronal MR image demonstrating supraspinatus pseudo-impingement. There is hypertrophy of the supraspinatus muscle with increased muscle bulk and paucity of intramuscular fat. Similar changes are seen in the other periarticular muscles. There is overfilling of the subacromial space by the hypertrophied distal muscle belly and myotendon with resultant secondary indentation of these structures by the overlying acromion and AC joint, resulting in clinical features of impingement..
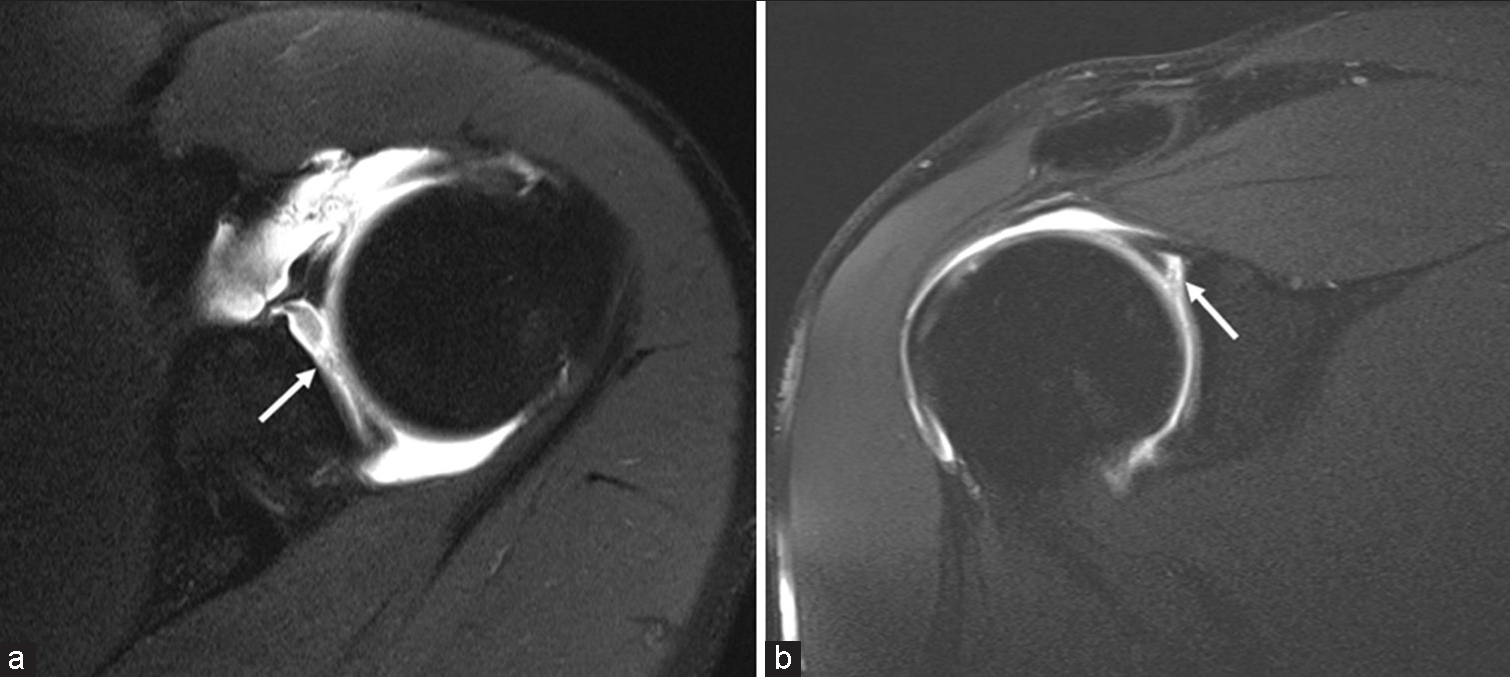
- A 41-year-old male presenting with shoulder pain. T1-weighted fat-saturated (a) axial and (b) coronal magnetic resonance arthrogram images demonstrating a superior labral tear (SLAP Type 3) involving its anteroposterior extent (white arrows).
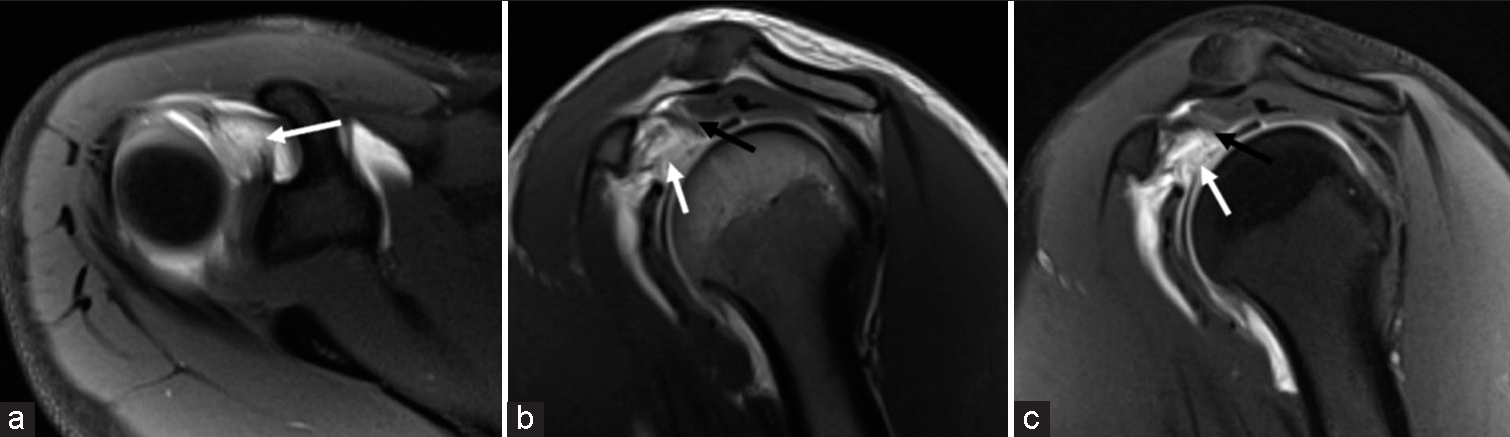
- A 19-year-old female presenting with shoulder pain following an injury during weightlifting training. T1-weighted fat-saturated (a) axial, (b) + (c) sagittal magnetic resonance arthrogram images demonstrating a full thickness tear of the superior glenohumeral ligament (SGHL) with discontinuity of the SGHL fibers (white arrows). The intact coracohumeral ligament is thickened and inhomogenous (black arrows). The SGHL and coracohumeral ligament together form the biceps pulley, which stabilizes the long head biceps tendon and glenohumeral joint.
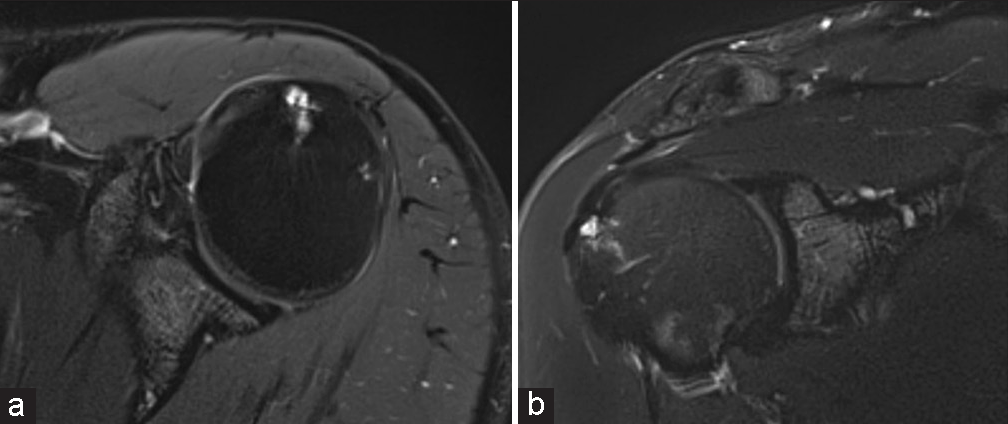
- A 19-year-old female presenting with shoulder pain following an injury during weightlifting training. T1-weighted fat-saturated (a) coronal and (b) sagittal magnetic resonance arthrogram images demonstrating a complete rupture of the entire anteroposterior extent of the inferior glenohumeral ligament (IGHL)/ capsule complex from the humeral attachment. Note the disruption of the “U”-shaped IGHL/capsule complex fibers (white arrows) from the humeral attachment with the resultant extracapsular extension of intraarticular gadolinium contrast (white arrowheads), confirming the capsular injury.
- A 40-year-old male presenting with focal shoulder pain following an injury during strength training. T2-weighted fat-saturated (a) coronal and (b) sagittal magnetic resonance images demonstrating lateral clavicle marrow edema seen as T2 signal hyperintensity (white arrows). This is likely on the basis of trabecular stress injury from weightlifting mechanics. There is also a sprain of the adjacent inferior acromioclavicular joints capsule-ligament complex.
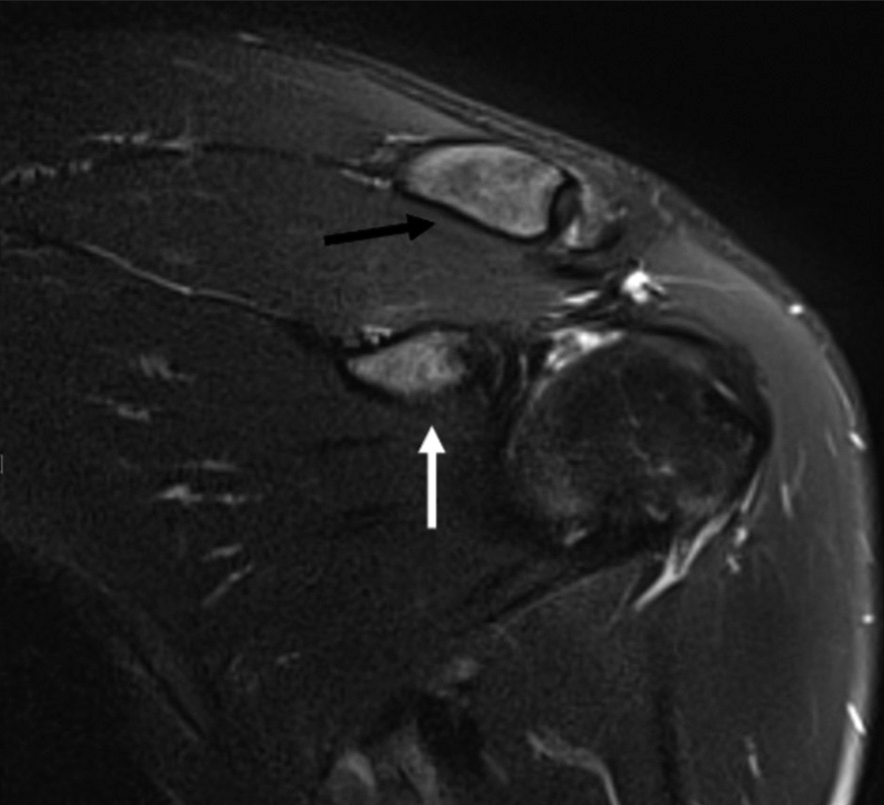
- A 36-year-old male presenting with shoulder pain. T2-weighted fat-saturated coronal magnetic resonance image demonstrating a coracoid process stress reaction. There is bone marrow edema of the coracoid process (white arrow) and lateral clavicle marrow edema (black arrow).
- A 39-year-old male presenting with shoulder pain. T2-weighted fat-saturated (a) axial and (b) coronal magnetic resonance images demonstrating traction cysts at the greater tuberosity of the humerus at the attachment of the supraspinatus tendon with surrounding marrow edema.
Knowledge of the biomechanics, injury patterns, and MRI appearances of weightlifting injuries, in conjunction with the clinical history of weightlifting regimens, can help with an accurate diagnosis of the underlying cause of shoulder pain and limitation of movement.
These shoulder injuries can have serious implications on an athlete’s function, performance, and return to sport. With weightlifting becoming a popular feature of strength-training programs, even in amateur athletes, the risk of shoulder injuries would undoubtedly rise.
CONCLUSION
This pictorial assay, therefore, aims to familiarize radiologists and sports physicians with MR patterns of shoulder/shoulder-girdle injuries to ensure the detection and timely treatment of weightlifting injuries.
Authors Contribution
All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Ethical approval
The research/study complied with the Helsinki Declaration of 1964.
Declaration of patient consent
Patient’s consent not required as patient’s identity is not disclosed or compromised.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The author(s) confirms that there was no use of Artificial Intelligence (AI)-Assisted Technology for assisting in the writing or editing of the manuscript and no images were manipulated using the AI.
Financial support and sponsorship
Nil.
References
- Resistance training for children and adolescents. Transl Pediatr. 2017;6:137-43.
- [CrossRef] [PubMed] [Google Scholar]
- The intensity and effects of strength training in the elderly. Dtsch Arztebl Int. 2011;108:359-64.
- [CrossRef] [PubMed] [Google Scholar]
- Unique aspects of competitive weightlifting: Performance, training and physiology. Sports Med. 2012;42:769-90.
- [CrossRef] [PubMed] [Google Scholar]
- Injuries and overuse syndromes in powerlifting. Int J Sports Med. 2011;32:703-11.
- [CrossRef] [PubMed] [Google Scholar]
- Olympic weightlifting training improves vertical jump height in sportspeople: A systematic review with meta-analysis. Br J Sports Med. 2016;50:865-72.
- [CrossRef] [PubMed] [Google Scholar]
- Strength training in soccer with a specific focus on highly trained players. Sports Med Open. 2015;1:17.
- [CrossRef] [PubMed] [Google Scholar]
- Core muscle activity during the clean and jerk lift with barbell versus sandbags and water bags. Int J Sports Phys Ther. 2015;10:803-10.
- [Google Scholar]
- Current concepts of muscle and tendon adaptation to strength and conditioning. Int J Sports Phys Ther. 2015;10:748-59.
- [Google Scholar]
- Resistance training is medicine: Effects of strength training on health. Curr Sports Med Rep. 2012;11:209-16.
- [CrossRef] [PubMed] [Google Scholar]
- Injury rates and profiles of elite competitive weightlifters. J Athl Train. 1999;34:232-8.
- [Google Scholar]
- Injuries among weightlifters and powerlifters: A systematic review. Br J Sports Med. 2017;51:211-9.
- [CrossRef] [PubMed] [Google Scholar]
- The Biomechanics and Applications of Strongman Exercises: A Systematic Review. Sports Med Open. 2019;5:49.
- [CrossRef] [PubMed] [Google Scholar]
- Weightlifting overhead pressing derivatives: A review of the literature. Sports Med. 2019;49:867-85.
- [CrossRef] [PubMed] [Google Scholar]




