
Translate this page into:
Middle-aged woman with chronic right hip and groin pain

*Corresponding author: Shrishail Adke, Department of Radiology, Deenanath Mangeshkar Hospital, Pune, Maharashtra, India. shri.adke@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Adke S, Desai S. Middle-aged woman with chronic right hip and groin pain. Indian J Musculoskelet Radiol. 2025;7:137-8. doi: 10.25259/IJMSR_71_2024
PART 1: QUESTION
Clinical history
A 40-year-old female presents with a 9-month history of right hip and groin pain. Identify the pathology.
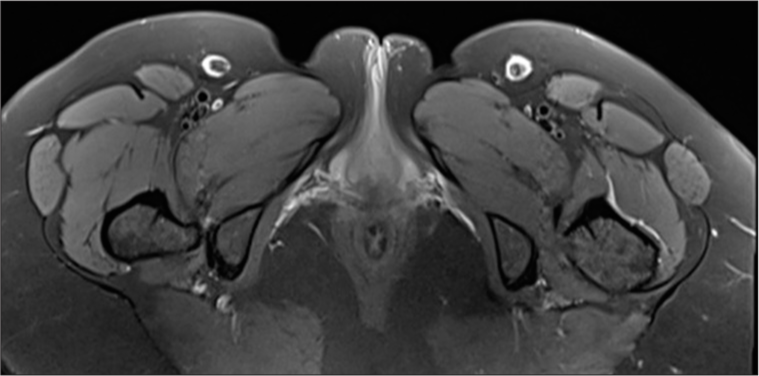
- Axial proton density fat saturation (PDFS) image of pelvis.
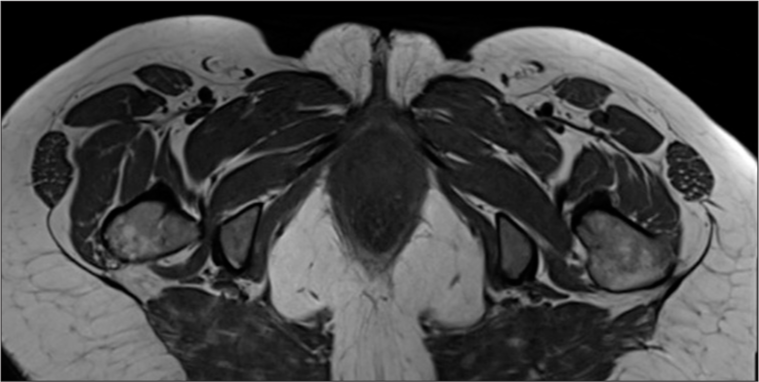
- Axial T1 image of pelvis.
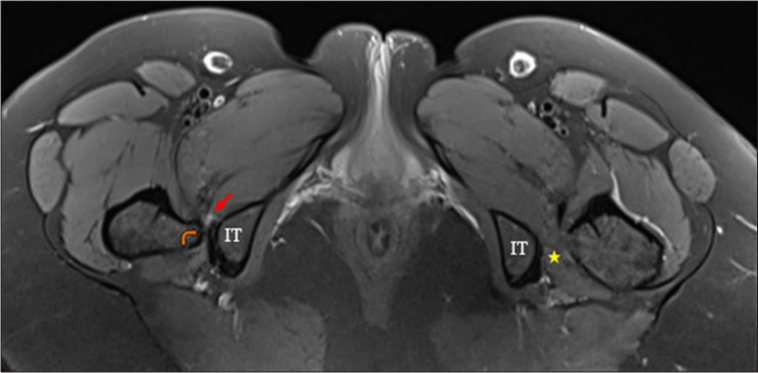
- Axial PDFS image of the pelvis demonstrates right ischiofemoral narrowing (orange curved arrow) with severe quadratus femoris muscle compression and edema (red arrows) and normal ischiofemoral space on the left side (yellow star). IT: Ischial tuberosity, PDFS: Proton density fat saturation
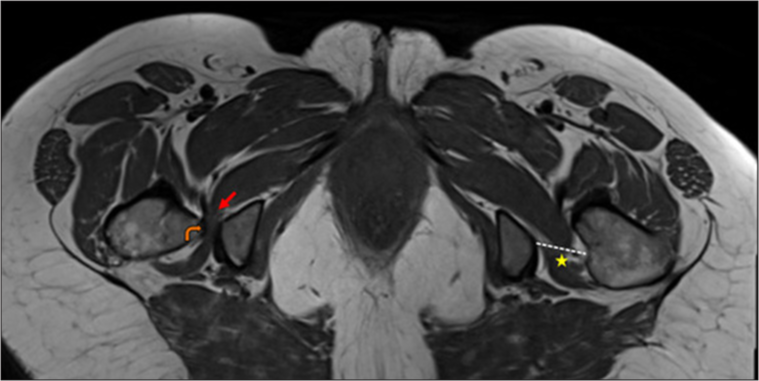
- Axial T1 image of pelvis demonstrates right ischiofemoral narrowing (orange curved arrow) with severe quadratus femoris muscle compression and atrophy (red arrows) and normal space on the left side (yellow star and dashed white line).
PART 2: ANSWER
Findings
Diagnosis: Right ischiofemoral impingement.
DISCUSSION
Ischiofemoral impingement (IFI) occurs when soft tissues, especially the quadratus femoris muscle (QFM), are compressed between the ischial tuberosity and the lesser trochanter of the femur.[1] This impingement is typically caused by a congenital or acquired narrowing of the ischiofemoral space, defined as the shortest distance between the medial cortex of the lesser trochanter and the lateral cortex of the ischial tuberosity. The normal width of this space is around 2 cm, with a threshold of approximately 15 mm considered indicative of narrowing.[2] IFI is often seen in middle-aged to elderly women and is a common source of hip, groin, and/or posterior thigh pain. As QFM is located in close proximity to the sciatic nerve, pressure effects may produce nerve-related symptoms. In acute cases, the QFM may show signs of edema or tears, while chronic cases reveal fatty atrophy. In addition, some patients may develop adventitious bursitis or a bursa-like fluid collection around the lesser trochanter.[3] Bone marrow edema or cystic changes in the ischium or lesser trochanter may also be evident. While magnetic resonance imaging (MRI) is an essential tool for diagnosing IFI, it is important to note that not all patients with ischiofemoral narrowing or muscle edema will experience symptoms. Furthermore, MRI should not be performed with the hip in external rotation, as this position can lead to an overestimation of the degree of space narrowing.[2]
DIFFERENTIAL DIAGNOSIS
QFM tear
Adductor/Hamstring muscle injury
Snapping hip syndrome
Piriformis syndrome
Lumbar radiculopathy.
TREATMENT
The initial approach to managing IFI is generally conservative, focusing on rest, activity modification, and the use of non-steroidal anti-inflammatory drugs to alleviate pain and inflammation.[4] In cases where conservative measures fail, computed tomography-guided injections of the QFM with a combination of local anesthetic and corticosteroid have demonstrated potential for providing long-term pain relief. For patients who do not respond to these noninvasive treatments, surgical options may be considered. Surgical interventions may involve the removal of inflamed or bursal-type tissue or, in more severe cases, excision of part of the lesser trochanter to relieve impingement and restore mobility.[5]
Acknowledgment
We acknowledge the help extended by Dr. Stanzin Spalkit in editing the manuscript.
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship: Nil.
References
- Ischiofemoral impingement: Evaluation with new MRI parameters and assessment of their reliability. Skeletal Radiol. 2012;41:575-87.
- [CrossRef] [PubMed] [Google Scholar]
- Ischiofemoral impingement syndrome: A meta-analysis. Skeletal Radiol. 2015;44:831-7.
- [CrossRef] [PubMed] [Google Scholar]
- Ischiofemoral impingement syndrome: An entity with hip pain and abnormalities of the quadratus femoris muscle. AJR Am J Roentgenol. 2009;193:186-90.
- [CrossRef] [PubMed] [Google Scholar]
- Evaluation and management of ischiofemoral impingement: A pathophysiologic, radiologic, and therapeutic approach to a complex diagnosis. Skeletal Radiol. 2016;45:771-87.
- [CrossRef] [PubMed] [Google Scholar]
- CT-guided infiltration of the ischiofemoral space in young patients with ischiofemoral impingement is an effective diagnostic tool. Insights Imaging. 2024;15:235.
- [CrossRef] [PubMed] [Google Scholar]




