
Translate this page into:
Pattern of Injuries in Indian Wrestlers

*Corresponding author: Shalini Agarwal, Department of Radiodiagnosis, Pandit Bhagwat Dayal Sharma, Post Graduate Institute of Medical Sciences, Rohtak, Haryana, India. Mobile: +91-9355622099. dragarwalshalini@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Agarwal S, Chhikara E, Rohilla RK. Pattern of Injuries in Indian Wrestlers. Indian J Musculoskelet Radiol 2020;2(2):97-103.
Abstract
Objectives:
Wrestling is a popular sport the world over. As one of the sports played during the Olympic games, it sees high player participation at both school and scholastic levels. However, player to player contact and its arduous nature leads to a high incidence of injuries. In spite of this, it has received little attention, especially with respect to injury rate in the Indian wrestlers. Hence, our aim was to study their pattern in these wrestlers.
Material and Methods:
We performed an observational study involving 190 wrestlers who were followed up over a period of 2 years. Their injuries were studied by means of a structured questionnaire, which they filled up with assistance from their athletic trainers.
Results:
A total of 184 injuries occurred in 190 wrestlers (≥16 years) with an injury rate of 5.08/1000 athlete exposure (A-E). There were 47.83% new injuries, while 52.1% were recurrent. Injuries that occurred during practice sessions were more than those during competitions. Most injuries occurred to the knee joint, followed by the shoulder joint. Ligament sprains and muscular strains were the most frequent injuries. Wrestlers practicing Freestyle (FS): Greeco-roman (GR) was 5.3:1. Statistically significant injuries to the trunk occurred in those practicing FS style. Ten wrestlers were operated for knee injuries.
Conclusion:
Indian wrestlers are at risk of higher injury rates, with the majority being recurrent and occurring mostly in practice sessions. The knee joint is most commonly involved, followed by the shoulder. FS is the preferred style and more commonly associated with trunk injuries. The goal of our study was to study the pattern of injuries in the Indian wrestler and to minimize the risk of injury by understanding the factors responsible.
Keywords
Wrestling
Indian
Freestyle
Greeco-roman
Injuries
Incidence density ratio
Injury proportion rate
Competitions
practice
Injury prevention

INTRODUCTION
Wrestling has been practiced since ancient times, and it is a popular sport in India. Conventionally, it is practiced in ashrams or akhadas on a field of dug earth and has been called “Mall yudh” or “Pehlwani.” More modern practices are being followed in recent times. The world over, records of ancient Olympic wrestling can be found as far back as 708 B.C.[1] It is a contact sport and its arduous nature, and compulsory physical contact leads to high injury rate.[2] Wrestling is second only to tackle football for the frequency of injury in high school athletes. This is in spite of having the sixth-highest average annual participation of boys in high school sports.[3]
This sport involves all parts of the body in voluntary and involuntary movements. Various biomechanical forces are imposed on both athletes due to the very nature of this game, leading to injury to different parts of the body.[1] The frequency and severity of these injuries depend on several factors and are the result of their interaction at a point in time. These factors are the type of exposure (competition vs. practice), style of wrestling, gender, age, etc. Hence, to record reliable epidemiological data, it is essential to determine these accurately. This is the first step towards building effective injury prevention program.[4]
Two styles; freestyle (FS) and Greco-roman (GR) are practiced the world over in the present time. The difference lies in the type of moves allowed. Holds and attacks are allowed to both the upper and the lower extremity in FS wrestling, whereas the lower extremity attacks are not allowed in GR type.[5] These are associated with a different pattern of injuries as a result. In India, FS is the more popular style. In the study that we present, all wrestlers started their careers practicing this style and shifted to GR style on sustaining injuries to the lower limb.
The popularity of this sport in India is evident from the number of medals won in Olympic and World championships by Indian wrestlers. In spite of this, Indian wrestling has received little attention in the world literature. The aim of this study was to evaluate the pattern of injuries experienced by the Indian wrestlers.
MATERIAL AND METHODS
We obtained permission from the institutional postgraduate board of studies and institutional ethics committees. All the participants also gave informed consent for the study, which was according to the guidelines laid down by the Declaration of Helsinki for human experiments.
Study design
This was an observational descriptive study. It was conducted over a 2 years period and included wrestlers from the largest akhada/wrestling school of the city.
Study population
One hundred and ninety wrestlers, aged 16 years or more, were studied. No pre-enrollment screening was performed. All the participants were provided with a structured questionnaire, which included player information such as weight, height, and duration, for which the player had been practicing and the style of wrestling (FS or GR) in addition to date of injury, the type of injury (whether new or recurrent), clinical and radiological diagnosis, player position, playing surface, type of session, and date of return to sport. The questionnaire was provided in a paper form and was filled up with help from their coaches/athletic trainers. It was collected at the time of each injury. In addition, we also obtained a weekly report from the athletic trainers regarding the injuries sustained by the wrestlers and wrestling hours of each wrestler (which were divided into match and competition). We then cross-checked these with each questionnaire submitted.
Clinical assessment and radiological investigations
All patients were clinically evaluated at the time of injury by different orthopedic surgeons as per the convenience of the players, and then appropriate radiological investigations were performed at our department, depending on the type of injury. The findings were then documented. Follow-up was performed depending on the severity of the wrestler’s symptoms until the wrestler returned to practice/competition or quit the game.
All radiographs were performed either on digital radiography system (Philips DD-2) or on computed radiography system (AFGA CR 75.0). Ultrasound was performed depending on the size of the patient. Computed tomography (CT) was done on Siemens Somatom Volume Zoom plus 4 spiral CT scanner. While, magnetic resonance imaging (MRI) was done on philips Gyroscan Intera Nova 1.5 Tesla MRI.
Operational definitions used in the study
Definitions of injury
Any significant condition that limited function of the wrestler, and prompted them to seek the help of professionals from the area of health. It could also be a condition that caused the abandonment of a fight or training and resulted in lost time from athletic participation for 1 day or more.
Recurrent injury
Any injury that occurs following an injury-free period, at the same body location, as an earlier injury. Recurrent injuries at the same site sustained during the period of study were included as recurrent injuries.
An athlete exposure (A-E)
It consists of one athlete participating in one wrestling practice or match.
Return to the game
Return of a wrestler to practice/ competition.
Follow-up was performed until a wrestler returned or quit the game.
Exclusion criteria
All old injuries sustained before the study period, those due to systemic diseases, soft-tissue or bony pathologies unrelated to the practice of wrestling, aggravation of previous injuries, all skin infections, and dental injuries related to wrestling.
Statistical analysis
We collected the data and analyzed it using SPSS software and EPINFO for Chi-square analysis. We calculated the injury rates as the ratio of injuries per 1000 athlete -matches.
The case rate per 100 players included multiple injuries to the same players as against the player rate per 100 players.
Incidence density ratio (IDR) = Game injury rate /practice injury rate.
Injury proportion rate (IPR) is as calculated by the following formula:
RESULTS
We studied 190 wrestlers aged 16 years and above (age range of 16–34 years; mean 19.92 years) weight range of 46–120 kg (mean wt = 69.82 kg) and height range of 140–195 cm (mean ht = 172.4 cm), practicing FS (160/190), and GR (30/190) type of wrestling.
These wrestlers sustained 184 injuries. There were 36592 athlete exposures in 119 injured wrestlers. Hence, the overall injury rate was 5.03 injuries/1000 athlete-exposures, while case rate/100 players and player rate/100 players were 0.95 and 0.63, respectively.
The number of new injuries was 88/184 (47.83%) and recurrent was 96/184 (52.10%). More recurrent injuries occurred in a defensive position in all age groups. However, the knee injuries were predominantly new and occurred predominantly in attack position. Those to the lower leg and ankle were predominantly accidental in nature.
The IDR of injuries was more for competitions. However, more number of injuries 85/119 (71.43%) occurred in practice sessions, while, only 34/119 (28.57%) injuries occurred in competitions. Injuries that occurred during practice sessions were during hard wrestling (65.73%) predominantly. The number of wrestlers who were injured in defense and attack position was 58/190 (30.53%), and 46/190 (24.21%), respectively, while 15/190 (7.89%) wrestlers sustained accidental injuries.
The maximum number of injuries was to the knee, i.e., 37.77% (71/184). Most of these occurred in the 20–24 years age group and in wrestlers practicing for 5–10 years [Figure 1]. The next joint to be involved commonly was the shoulder (18.62% of injuries) [Figure 2]. Ligamentous and muscular sprain and strain were the most common lesions in all age groups [Figure 3].
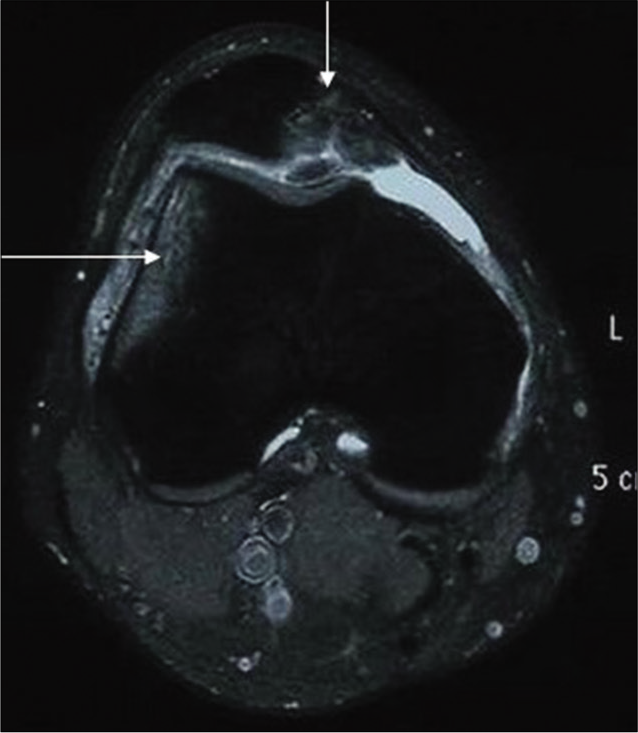
- Axial PD fat suppressed image reveals bone contusion involving lateral femoral condyle in a 20 years old wrestler (wt-90 kg, ht-180 cm, and duration of training 5 years) (long arrow) and osteochondral fracture along the medial facet of the patella (short arrow) suggesting a possibility of transient patellar dislocation. The injury occurred in competition and during defense position. He took conservative treatment for 3 months and was relieved.
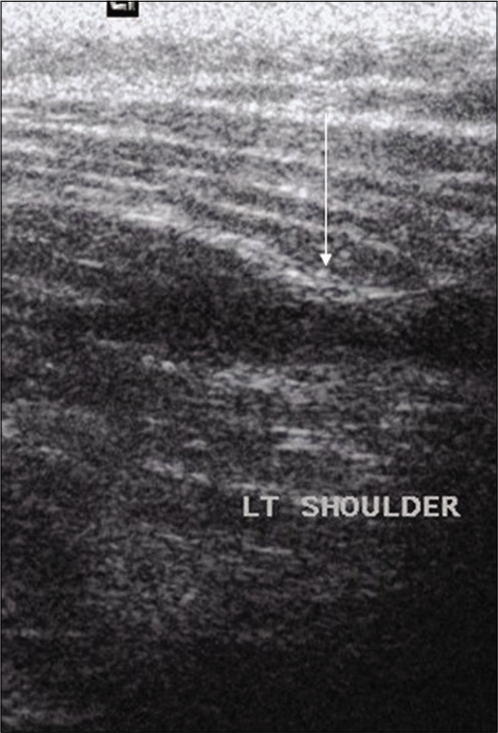
- US image reveals Grade II Strain of left deltoid muscle of a 19 years old wrestler (wt-80, ht-168 cm, and duration of training for 8 years), shows hypoechoic area (arrow) in the region of its posterior attachment. The patient sustained this injury during training (hard wrestling) in a defensive position (take down). He took conservative treatment for 1 month after which he got symptomatic relief. He did not report for a follow-up scan.
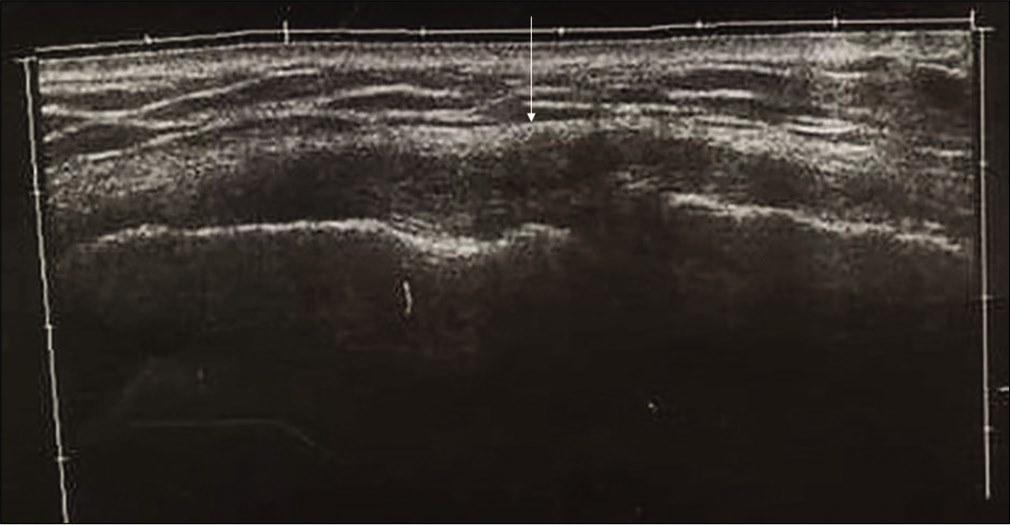
- Panoramic US image of 21 years old wrestler (wt-60 kg, ht-165 cm, and duration of training 7 years), shows thickening and hypoechogenicity of the medial collateral ligament (arrow). The injury occurred during training (hard wrestling) in defense position. He got complete symptomatic relief with 15 days of conservative therapy.
Trunk injuries (17/184) occurred more frequently in wrestlers practicing FS type of wrestling. This was statistically significant (P ≤ 0.029). Compared with GR wrestling, there was a greater proportion of knee injuries in FS wrestling (IPR = 1.37). In GR wrestling, there were a greater proportion of shoulder injuries (IPR = 0.70).
On comparing injuries with weight class, only elbow injuries (12/184) were found to be statistically significant occurring in the 70–79 kg [Figure 4], while wrist and hand injuries occurred most frequently in wrestlers with a height range of 150–179 cm (P = 0.00) [Figure 5].
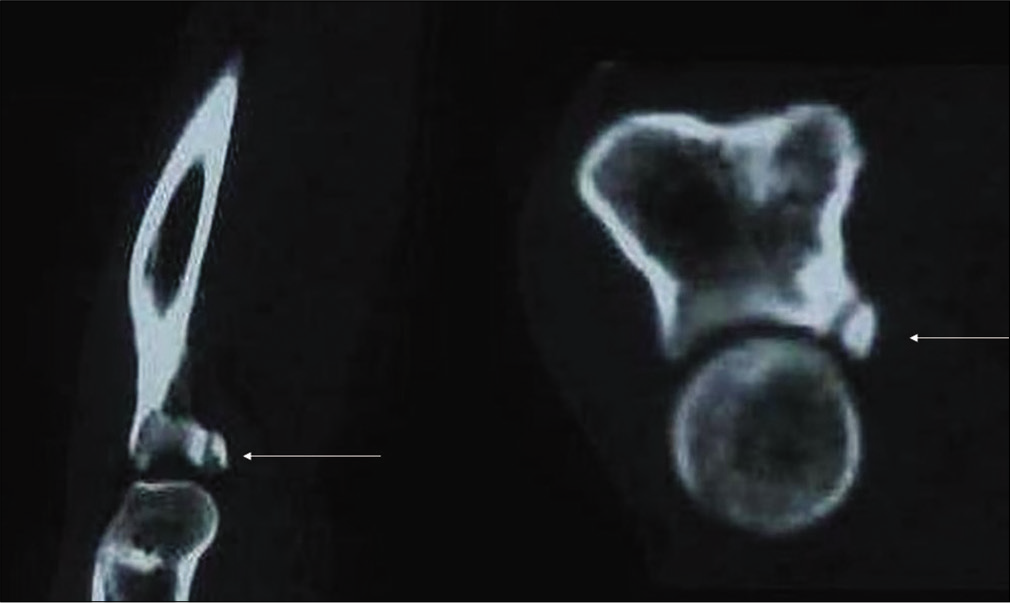
- Sagittal and coronal reconstructed computed tomography images of Rt elbow of a 20 years old wrestler (wt-75 kg, ht-153 cm, and duration of training for 7 years) show a chip fracture of coronoid process of Rt ulna (arrow). The wrestler sustained this injury during practice (hard wrestling) in attack position.
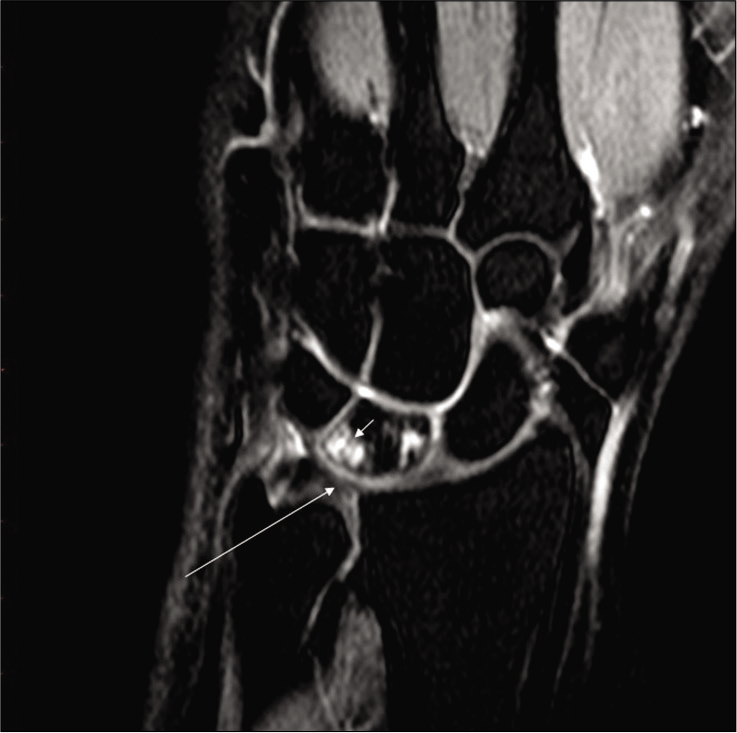
- Coronal PD weighted fat-suppressed image of the left wrist reveals negative ulnar variance with a contusion of lunate (arrowhead) and degeneration of TFCC (long arrow) in a 20 years old wrestler (wt-66 kg, ht-171 cm, and duration of training for 5 years). The wrestler had multiple episodes of pain involving his left wrist, for which he would just take conservative treatment with relief.
The relationship of injured wrestlers with the weight class and height is shown as pie charts [Figures 6 and 7].
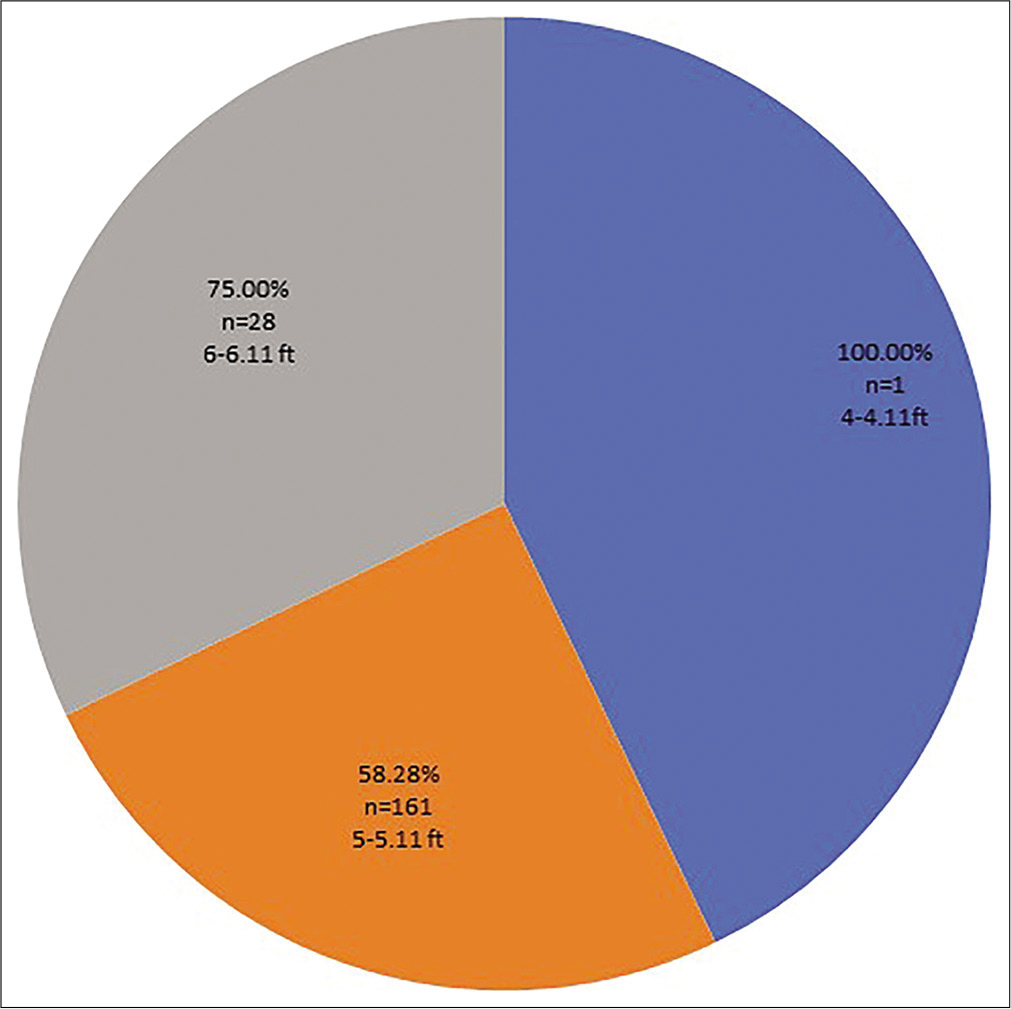
- Pie chart depicting the relationship between the injured wrestlers and their height.
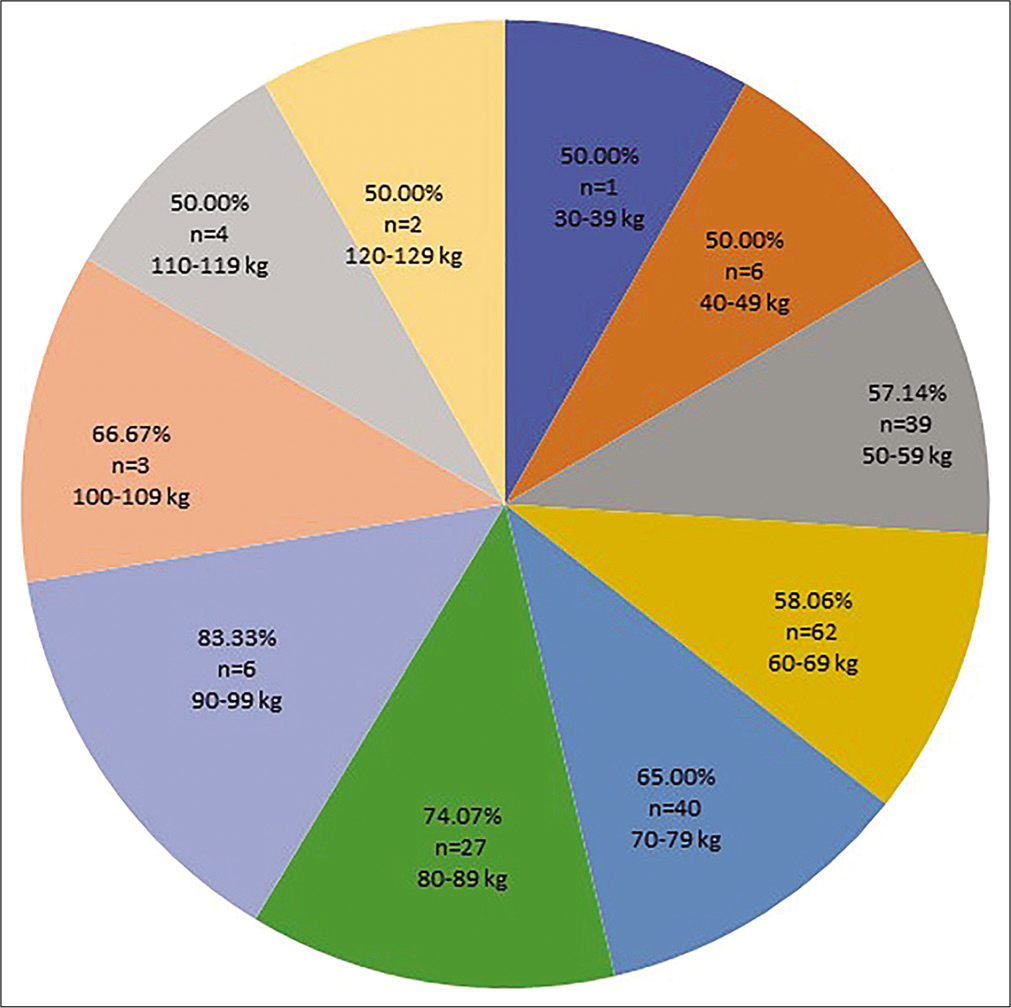
- Pie chart depicting the relationship between the injured wrestlers and their weight.
Most injured wrestlers (48/62; 77.42%) had been practicing for 5–10 years. The next commonly injured group had been practicing for 11–15 years (4/7; 57.14%). Knee injuries and lower leg and foot injuries [Figure 8] were positively correlated with the duration of practice.
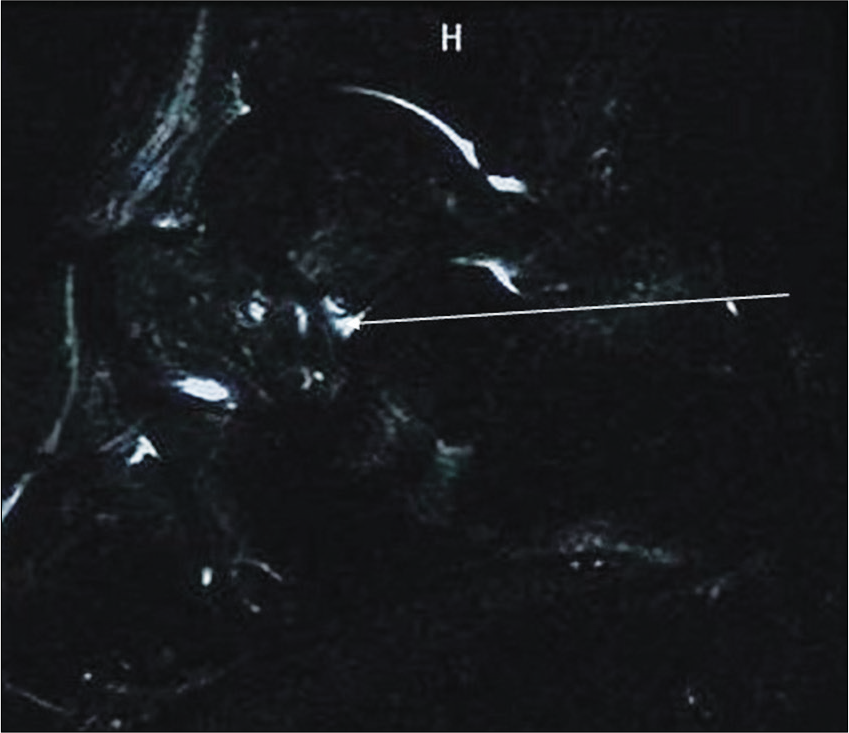
- STIR Image of a 19 years old wrestler (wt-62 kg, ht-171 cm, and duration of training 3 years) shows altered signal intensity in the region of sinus tarsi (long arrow). There is also mild effusion in the subtalar joint space. The wrestler sustained this injury in a practice session (drill).
More wrestlers, i.e., 105 were treated conservatively, while 10/190 wrestlers underwent operative treatment. All the wrestlers who underwent operative treatment returned only after 1 month, while the majority took less than a week to return to the game.
DISCUSSION
Wrestling is associated with a high rate of injury. For all games, football has been consistently found to have the highest rate of injury (35.9/1000A-Es), with wrestling close behind (26.4/1000 A-Es).[6] Jarret et al. analyzed the injuries which occurred over an 11-year period in National College of Athletic Association (NCAA) sports and found that wrestling finished second only to spring football for the highest rate of injury at 9.6 injuries/1000 A-Es.[7] Kordi et al. reported an injury rate of 5.7 injuries/1000 wrestling exposures in 129 wrestlers over a period of 1 year,[8] while Myers et al. found the annual cumulative injury incidence to be 29.57 injuries/1000 wrestlers/year in the scholastic group.[9] Barroso et al. found that 85.3% of all musculoskeletal injuries in athletes resulted from wrestling.[2] The overall rate of injury was 5.13 injuries/1000 A-Es in our study.
In the study by Kordi et al., new injuries were most common (77%), followed by recurrent (10%) and unresolved injuries (2%) from the preceding year, while 1% were due to recent worsening of an unresolved injuries.[8] Pasque et al. reported an incidence of 6% for a re-aggravation of previous injuries.[10] In a study by Mysnyk et al., 8/13 athletes suffering from pre-patellar bursitis had at least one recurrence.[11] There were 47.83% new injuries in our study, while 52.1% were recurrent.
A longer length of practice has been associated with greater occurrence of injuries.[2] Pasque et al. reported similar findings in their study on high school wrestlers. Varsity wrestlers comprised 44% of their study population but suffered 60% of the injuries. This can be explained by a more aggressive style of wrestling.[10] In our study, most injured wrestlers (48/62; 77.42%) had been practicing for 5–10 years, while the next commonly injured group had been practicing for 11–15 years (4/7; 57.14%). Knee injuries, and lower leg and foot injuries were positively correlated with the duration of practice.
The defensive wrestler is more likely to be off-balance, and hence they are particularly at risk. They also may have one or both arms held and there is a high probability of their opponent falling on top of them. In a situation such as this, the wrestler is likely to land on his head and twist his neck.[12] Jarret et al.[7] eported “takedown” as the most common mechanism of injury, and Agel et al.[13] found it to be “player contact.” Boden et al.[12] also found the defensive position to be most frequently associated with the injury. In their study, the “takedown” maneuver was most commonly responsible for the injury (74%), followed by down position (23%) and lying position (3%).[2] More number of wrestlers, i.e., 58/119 (48.7%) were injured in a defensive position in our study as well.
Injury rates have been found to be significantly higher in games. Hootman et al.[6] studied the epidemiology of collegiate injuries in 15 sports and found statistically higher injuries in games (13.8 injuries/1000 A-Es) than in practices (4.0 injuries/1000A-Es). In practice, the non-contact injury mechanism was 36.8% of all injuries. This trend was twice as common as in games. According to the study by Boden et al.,[12] 80% of wrestling injuries occurred in match competitions. Pasque et al.[10] reported that 63% of their injuries occurred in practice, while only 37% occurred during competition. IDR for injuries in games was higher in our study as well; however, more number of injuries occurred in practice sessions and during hard wrestling.
Akbarnejad et al. reported that on comparing injuries between wrestlers practicing GR and FS styles; wrestlers practicing GR style were injured more frequently (66.67%),[1] While Yard et al. reported significantly higher rates of tournament injuries in wrestlers practicing FS style.[14] Akbarnejad et al. found that wrestlers practicing FS style wrestling were at a higher risk of head and neck, trunk, upper extremity, and lower extremity injuries compared to those practicing GR style.[1] There were more number of wrestlers practicing FS style in our study, and they sustained more number of trunk injuries which was statistically significant.
Cohen et al. proposed that wrestling injuries should be divided into contusions, fractures, dislocations, sprains, muscle lesions, and tendinitis. In terms of location, they further divided them into lower limbs (thigh, knee, leg, ankle, and foot), upper limbs (shoulder, arm, elbow, forearm, wrist, and hand), and trunk.[15] In a study by Yard et al.,[5] lacerations and cartilage injuries were the most common injuries in college wrestlers. Pappas[16] reported sprains/ strains (36.5%) and fractures (21.3%) and Jarret et al.[7] report sprain, strains, and contusions as the most common injuries.
Knee, face, shoulder, ankle, and neck were the common sites injured in a study by Hewett et al. According to them, most injuries occurred due to player contact, or contact with the mat or due to twisting forces.[17] Large joints such as shoulder and knee are more commonly involved in scholastic wrestlers, while fingers, wrist, hand, head, and neck are involved in case of injuries sustained by youth wrestlers.[17] No such distinction was noted in our study. Knee injuries were most common in our study, and this was followed by the injuries to the shoulder. In an earlier study published by us, we found that more injuries to the knee were new and occurred in attack position.[18]
Knee injuries were highest in number in a study by Barroso et al., followed by the shoulder (20%).[2] Knee was the most common joint involved in our study as well. Park et al. studied 238 elite Korean wrestlers and found that the most number of injuries occurred to the lower extremity, followed by the upper extremity, trunk, and head and neck area.[19]
Most studies have found no statistically significant relationship between injury and weight class. However, Boden et al. found that more injuries occurred in the lowand middle-weight classes.[12] No statistically significant difference was found in our study between injuries and weight class except for the injuries to the elbow (which occurred in 70–79 kg weight class). This needs to be correlated with further research in the future.
Authors could not find a universally accepted criterion for evaluation of the severity of sports injuries. Barroso et al.[2] assigned the need for surgical treatment as a severity parameter. There were 9% lesions that had to be operated in their study, and most of these lesions were located in the knee. In our study, only ten wrestlers were operated, while the rest were conservatively managed. Agel et al.[13] have described a ratio of approximately 30% of severe injuries (more than 10 days’ recovery period). Boden et al.,[12] on the other hand, reported 2.11 catastrophic injuries per year. In their study over a period of 18 years, these injuries included 27 cervical fractures or major cervical ligament injuries, 4 spinal cord contusions with transient quadriparesis, 3 severe head injuries, and an acutely herniated disc. Several authors,[2] using different methods to evaluate severity, report that the majority of wrestling injuries are not considered severe.
Among the 10 study sports studied by Powell et al. wrestlers suffered the highest proportion of injuries for which a player missed more than 7 days, followed by baseball. The lowest proportion was for field hockey, and softball.[20] 10/190 wrestlers from our study group underwent operative treatment and were absent from the game for over a year.
CONCLUSION
There are several limitations of our study, such as ignorance regarding the importance of reporting these injuries and regular follow-up, broad selection criteria, and wide and nonuniform treatment options followed. The athletes tend to downplay the injuries sustained to not to lose time away from practice and games. They persist in treating these injuries by traditional methods and rarely seek proper medical attention. However, our study brings out certain vital aspects of the injury patterns of adult Indian wrestlers such as the high rate of injury, preferred style of wrestling, commonest joint involved, an association of trunk injuries with FS wrestling, the age group with maximum injuries, relationship with duration of practice, height, weight class, etc.
Each sport is associated with a characteristic injury profile. There are several causative factors; however, the effect depends on the interaction of these factors at that point in time when an injury occurs. An understanding of these helps in the formulation of an effective injury prevention program. Authors could not find any such study on Indian wrestlers who practice under conditions that are very different from those of the wrestlers reported in the literature so far. Further research must be taken up in this area to give these wrestlers a better chance in the international arena.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Frequency of sports trauma in elite national level greco-roman wrestling competitions. Arch Trauma Res. 2012;1:51-3.
- [CrossRef] [PubMed] [Google Scholar]
- Musculoskeletal injuries in Wrestling Athletes. Acta Ortop Bras. 2011;19:98-101.
- [CrossRef] [Google Scholar]
- High school injury surveillance systems In: Proceedings of Sports Injuries in Youth: Surveillance Strategies. Bethesda, MD: National Institutes of Health; 1991.
- [Google Scholar]
- Youth sports anterior cruciate ligament and knee injury epidemiology: Who is getting injured? In what sports? When? Clin Sports Med. 2011;30:691-706.
- [CrossRef] [PubMed] [Google Scholar]
- An epidemiologic comparison of high school and college wrestling injuries. Am J Sports Med. 2008;36:57-64.
- [CrossRef] [PubMed] [Google Scholar]
- Epidemiology of collegiate injuries for 15 sports: Summary and recommendations for injury prevention initiatives. J Athl Train. 2007;42:311-9.
- [Google Scholar]
- Injuries in collegiate wrestling. Am J Sports Med. 1998;26:674-80.
- [CrossRef] [PubMed] [Google Scholar]
- Sports injuries and health problems among wrestlers in Tehran March. J Pak Med Assoc. 2012;62:204-8.
- [Google Scholar]
- Competitive wrestling-related injuries in school aged athletes in US Emergency departments. West J Emerg Med. 2010;11:442-9.
- [Google Scholar]
- A prospective study of high school wrestling injuries. Am J Sports Med. 2000;28:509-15.
- [CrossRef] [PubMed] [Google Scholar]
- Prepatellar bursitis in wrestlers. Am J Sports Med. 1986;14:46-54.
- [CrossRef] [PubMed] [Google Scholar]
- Catastrophic Injuries in wrestlers. Am J Sports Med. 2002;30:791-5.
- [CrossRef] [PubMed] [Google Scholar]
- Marshall SW Descriptive epidemiology of collegiate men's wrestling injuries: National collegiate athletic association injury surveillance system 1988-1989 through 2003-2004. J Athl Train. 2007;42:303-10.
- [Google Scholar]
- A comparison of pediatric freestyle and Greco-Roman wrestling injuries sustained during a 2006 US national tournament. Scand J Med Sci Sports. 2008;18:491-7.
- [CrossRef] [PubMed] [Google Scholar]
- Boxing, wrestling, and martial arts related injuries treated in emergency departments in the United States, 2002-2005. J Sports Sci Med. 2007;6:58-61.
- [Google Scholar]
- Knee injuries in wrestlers: A prospective study from the Indian subcontinent. Asian J Sports Med 19;. ;7:e35000.
- [CrossRef] [PubMed] [Google Scholar]
- Injuries in male and female elite Korean wrestling athletes: A 10-year epidemiological study. Br J Sports Med. 2019;53:430-35.
- [CrossRef] [PubMed] [Google Scholar]
- Injury patterns in selected high school sports: A review of the 1995-1997 seasons. J Athl Train. 1999;34:277-84.
- [Google Scholar]




