
Translate this page into:
Extensor carpi ulnaris longitudinal tear: An overlooked etiology of ulnar-sided wrist pain


*Corresponding author: Kanchan Nigam, Department of Radiodiagnosis and Interventional Radiology, Vardhman Mahavir Medical College and Safdarjung Hospital, New Delhi, India. drkanchan.rad@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Nigam K, Katyan A, Singh DK, Maggo K. Extensor carpi ulnaris longitudinal tear: An overlooked etiology of ulnar-sided wrist pain. Indian J Musculoskelet Radiol. 2024;6:36-9. doi: 10.25259/IJMSR_41_2023
Abstract
The common etiologies of ulnar-sided wrist pain include fracture, triangular fibrocartilage complex injury, ulnocarpal impaction, extensor carpi ulnaris tenosynovitis, and distal radioulnar joint instability. Early and precise diagnosis is the cornerstone for management and early recovery from the disease. A dual-modality approach with X-ray and ultrasound wrist can be used as an efficient and cost-effective screening procedure for ulnar-sided wrist pain in a busy tertiary care setting or where magnetic resonance imaging is not available. We report a case of a 36-year-old male with chronic ulnar-sided wrist pain.
Keywords
Extensor carpi ulnaris tendon tear
Triangular fibrocartilage complex tear
tenosynovitis

INTRODUCTION
The primary mechanism of ulnar-sided wrist injury is increased axial loading of the forearm. This usually occurs due to a fall on an outstretched hand, which may lead to fracture, injury to triangular fibrocartilage complex (TFCC), injury to the extensor carpi ulnaris (ECU) tendon, and distal radioulnar joint instability. ECU split tears are present in 64% of anatomical specimens.[1] Imaging plays a key role in pinpointing the exact site of injury, which further determines specific management. Plain radiographs and magnetic resonance imaging (MRI) are the primary modalities for imaging evaluation of ulnar-sided wrist pain. Ultrasound (USG) of the wrist is a recently recognized cost-effective imaging modality in diagnostic evaluation and interventional management of pathologies affecting the ulnar side of the wrist.
We report a case of an adult male presenting with chronic ulnar-sided wrist pain in which USG determined imaging findings, in addition to plain radiographs and MRI, altered the final management of the patient.
CASE REPORT
A 36-year-old male, a carpenter by profession, presented to our hospital with pain in the ulnar aspect of the right wrist for the past three months, which aggravated supination-pronation movements. There was a history of twisting injury of the right wrist three months ago. No substantial relief in symptoms was observed by conservative management, which included ice packs, immobilization, and analgesics.
A plain radiograph of the right wrist in the dorsovolar view demonstrated no osseous abnormality [Figure 1]. MRI was performed based on the clinical suspicion of TFCC injury, but TFCC was normal [Figures 2a and b], while a long segment T2W hyperintensity was observed within the ECU tendon sheath, suggestive of tenosynovitis [Figures 3a and b]. Magnetic resonance (MR) signs of ECU tendon injury were conspicuous by their absence. There was no evidence of ECU tendon subluxation. In view of clinical, radiographic, and MR findings, an imaging diagnosis of ECU tendon tenosynovitis was arrived at. The patient was planned for a USG-guided steroid injection into the ECU tendon sheath. Pre-interventional USG of the right wrist was performed using a 12–18 MHz linear transducer. Static USG demonstrated tenosynovitis with a longitudinal split tear in the distal ECU tendon at the level of the ulnar groove measuring approximately 4 cm in length [Figures 4a, b, and 5]. There was no evidence of retraction of ECU tendon fibers on USG. Dynamic USG of the wrist performed in supination and pronation showed no evidence of ECU tendon subluxation or sub sheath injury. A final diagnosis of longitudinal split tear of the ECU tendon without retraction along with tenosynovitis was arrived based on comprehensive imaging evaluation by radiograph, MRI, and USG. In view of new findings of tendon tear as detected on USG, the initial plan of management by USG-guided steroid therapy was withdrawn to avoid the risk of tendon rupture. On retrospective analysis of magnetic resonance images, a thin T1W isointense focus was seen in the ECU tendon substance. Due to a 3-month-old trauma history, this could suggest the possibility of a partially healed chronic ECU tendon tear. In view of these new findings, the patient was put in cast by an orthopedic surgeon for 21 days.

- Plain radiograph (dorsovolar view) of the right wrist showing normal osseous and articular structures.
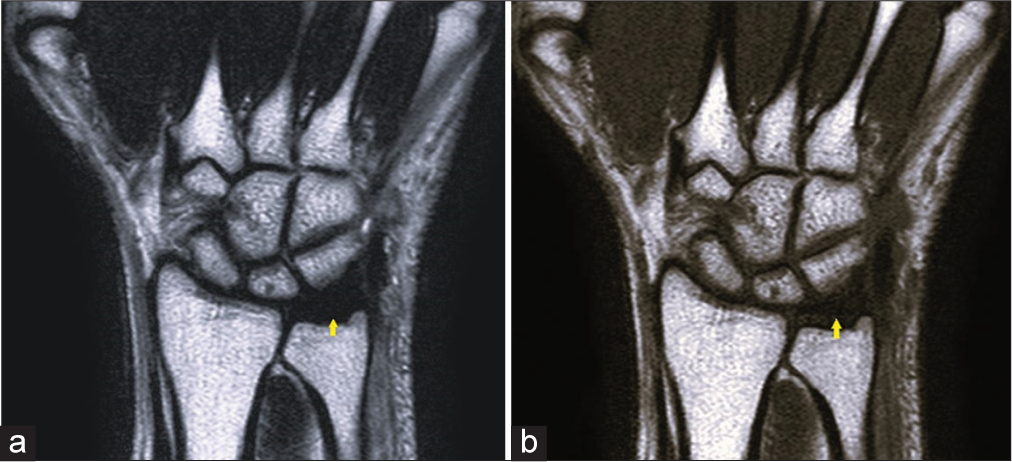
- (a) Coronal T2-weighted magnetic resonance (MR) images of the wrist demonstrate normal hypointense signal of the triangular fibrocartilage complex (TFCC) (yellow arrow). (b) Coronal T1-weighted MR images of the wrist demonstrate a normal hypointense signal of the TFCC (yellow arrow).
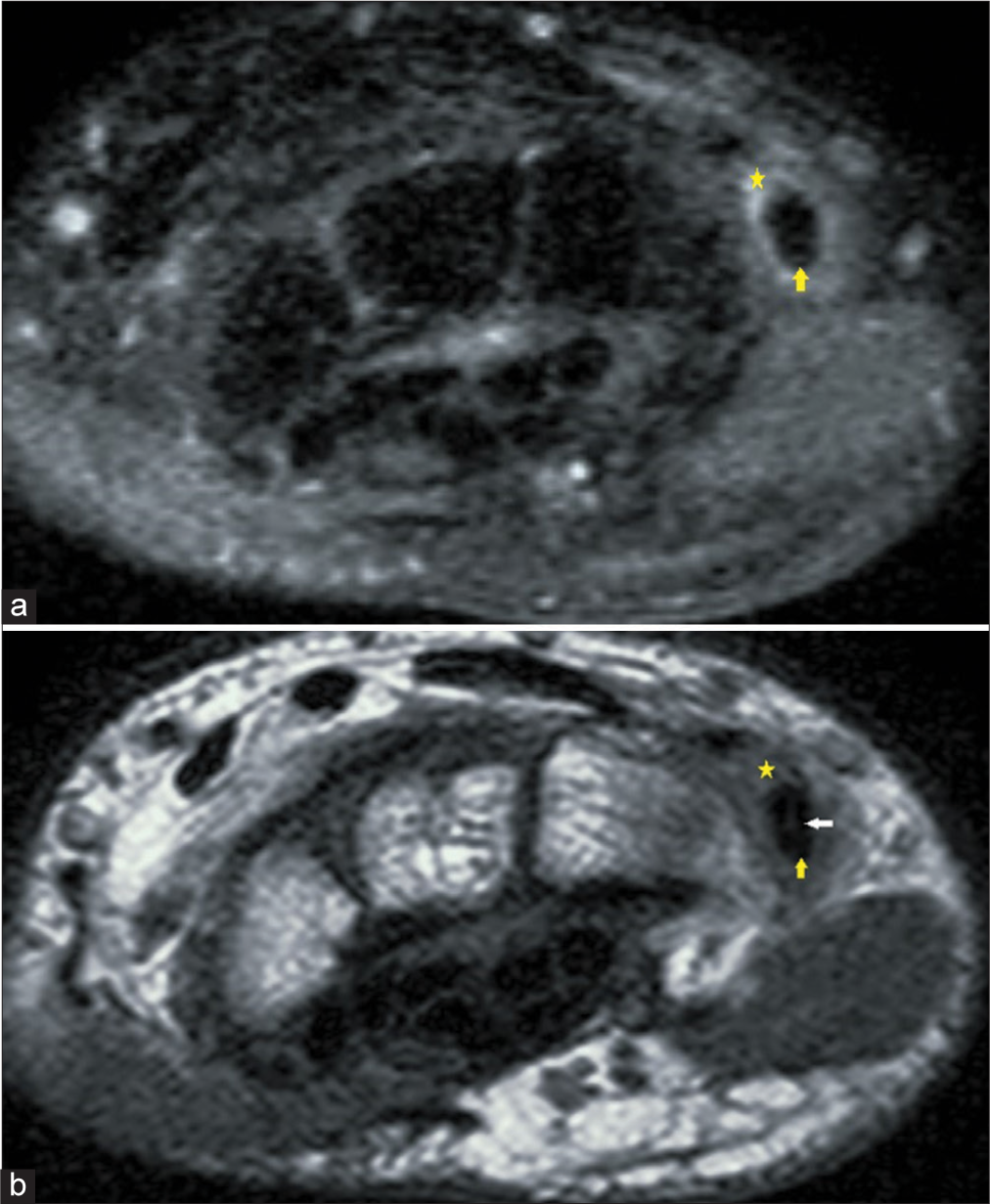
- (a) Axial proton density (PD) fat-saturated magnetic resonance (MR) images of the wrist demonstrate synovial thickening with fluid in the tendon sheath of extensor carpi ulnaris (ECU) (yellow asterisk). ECU tendon (yellow arrow) demonstrates normal signal intensity. (b) T1-weighted MR images of the wrist demonstrate synovial thickening with fluid in the tendon sheath of ECU (yellow asterisk). ECU tendon (yellow arrow) demonstrates normal low-signal intensity peripherally. A small T1 isointense focus is seen within the substance of the ECU tendon (white arrow), suggesting a chronic partially healed tear.
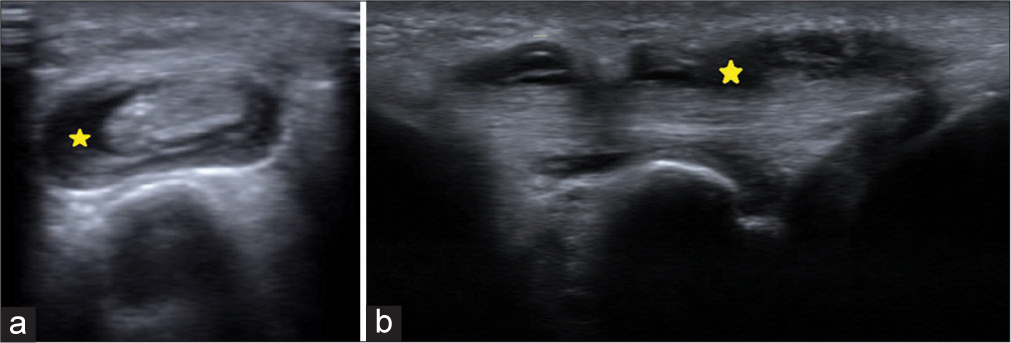
- (a) Ultrasound short-axis images of the wrist demonstrate synovial thickening with fluid in the tendon sheath of extensor carpi ulnaris (ECU) (yellow asterisk), consistent with ECU tenosynovitis. (b) Ultrasound long-axis images of the wrist demonstrate synovial thickening with fluid in the tendon sheath of ECU (yellow asterisk), consistent with ECU tenosynovitis.
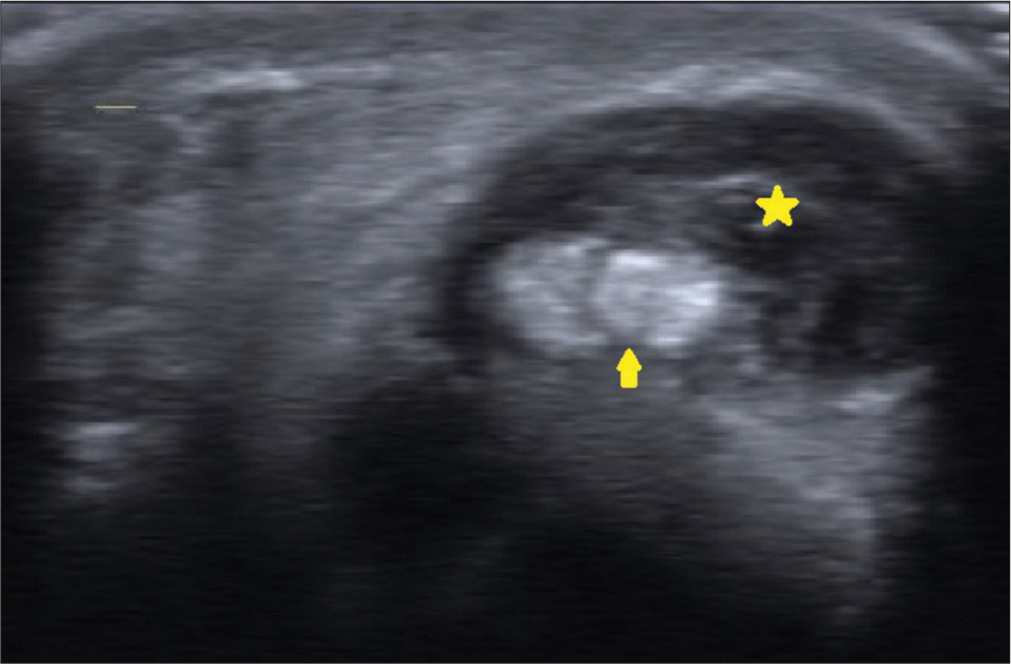
- Ultrasound of the short axis of the wrist demonstrates a full-thickness split tear of the extensor carpi ulnaris tendon (yellow arrow) with surrounding tenosynovitis (yellow asterisk).
DISCUSSION
Ulnar-sided wrist pain is a cause of significant morbidity, and a thorough clinical assessment along with comprehensive imaging evaluation can reliably differentiate these entities and guide further management.
TFCC comprises triangular fibrocartilage, volar and dorsal radioulnar ligament, meniscus homolog, ulnar collateral ligament, and ECU tendon sheath. Recent literature has also included ulnolunate and ulnotriquetral ligament as a part of TFCC.[2] The arrangement of TFCC and ulna has been found to provide 20% of axial loading of the forearm to the hand. Moreover, TFCC is the primary stabilizer of the distal radioulnar joint.[3] The mechanism of injury is rotation and compression of TFCC, which may occur either as an acute event or as chronic repetitive trauma. In addition, patients with positive ulnar variance are more prone to TFCC injury.
ECU originates from the lateral epicondyle of the humerus and inserts at the base of the fifth metacarpal. It lies in a bony groove on the dorsal surface of the ulna and leaves the wrist through a fibro-osseous tunnel. It is kept in position by a sub-sheath and retinaculum. This retinaculum prevents the bowstringing of the tendon during muscle contraction.[4] ECU stabilizes the distal radio-ulnar joint in supination and neutral position.[5] Repetitive flexion and extension of the wrist, especially in combined supination and flexion positions, can produce ECU tenosynovitis or tendinopathy. A negative ulnar variance, shallow ulnar groove, and a large ulnar styloid process also contribute to the development of ECU tendinopathy by mechanical irritation of the ECU tendon.[4] On the other hand, disruption of the ECU sub sheath produces tendon instability and subluxation.
Distinction between the various ECU pathologies can be aided by clinical history and examination–patients with stable ECU tendons have a gradual onset of symptoms, whereas those with unstable ECU typically have an acute onset of pain. Ulnar-sided wrist pain with difficulty in extension and ulnar deviation suggests ECU tendinopathy, whereas the presence of only weakness during extension without pain suggests rupture of the tendon. The ECU synergy test also helps distinguish between ECU pathology and other intraarticular pathologies.[4]
MRI of the wrist joint is usually the second step in the evaluation of ulnar-sided wrist pain after clinical examination. According to studies, the sensitivity of diagnosing ECU pathology on MRI is 57%[6], and for TFCC injury, it is 67 to 100%.[7] This shows that the efficacy of MRI in picking up ECU tendon tears is moderate and emphasizes the need for alternative imaging modalities like USG. A study on ECU injuries in tennis players by Montalvan et al. recommended both USG and MRI for imaging as they allow better identification of anatomical damage and healing.[8] USG has various advantages over MRI. It allows dynamic examination of the wrist in both supination and pronation positions in the same sitting. It also allows comparison of the normal side with the affected side. Apart from this, USG is a readily available, time-saving, and inexpensive modality compared to MRI.
Due to similar clinical presentation, injury to TFCC or ECU tendon can be difficult to differentiate on physical examination. However, the distinction between these two entities is paramount as management for both these conditions is different. For TFCC injury, USG-guided steroid injection is the treatment of choice and acts by decreasing inflammation. The established management protocol for ECU tendon tear without tenosynovitis is a USG-guided platelet-rich plasma (PRP) injection. PRP has growth factors that attract inflammatory agents to the site of injury and help in the healing process. If both tenosynovitis and tendon tear were to occur together, neither PRP nor depot injection could be administered. This is because the steroids would prevent the healing of tendon injury due to their anti-inflammatory properties and may even convert a partial-thickness tear into a full-thickness tear. On the other end, PRP injection would exaggerate the inflammation if tenosynovitis is present. Hence, it is imperative to make a precise diagnosis before commencing the treatment. In our patient, the MRI showed a normal TFCC with ECU tenosynovitis but failed to demonstrate the longitudinal split tear of the ECU tendon. On the basis of MR findings alone, steroid injection would have been the treatment of choice, which, if administered in this patient, may have led to a catastrophic outcome. High-resolution USG clinched the diagnosis of ECU tendon tear, which, in the presence of associated tenosynovitis, was an absolute contraindication for either steroid or PRP therapy.[9,10]
The surgical management of ECU tendons depends on the pathology involved. In case of ECU instability surgical repair is done in cases of acute traumatic ECU instability or in nonresponders (first-line management is the application of a cast in pronation, extension, and radial deviation for 6–8 weeks). In ECU tendinopathy, division of tendon with debridement of necrotic tissue can be attempted. In cases of ECU tendon rupture, reconstruction of the tendon with a palmaris longus graft has to be done.[8]
CONCLUSION
Imaging by MRI alone may provide a suboptimal evaluation of a patient presenting with ulnar-sided wrist pain and may overlook key diagnostic features. Incorporation of high-resolution USG into routine imaging assessment protocols along with MRI may provide a holistic approach to the evaluation of ulnar-sided wrist pain and guide proper management. Moreover, dynamic USG, by virtue of its easy availability and cost-effectiveness, in combination with X-ray, can be used in a busy OPD in a tertiary care setting where the waiting list for MRI is often long. It may also be useful in settings where MRI modality is not available to guide further management.
Acknowledgment
I want to thank my consultants and peers for their guidance and input in making this possible.
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
Patient’s consent is not required as patients identity is not disclosed or compromised.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Extensor carpi ulnaris tendon anatomy may mimic tears. J Hand Surg Asian Pac Vol. 2019;24:175-9.
- [CrossRef] [Google Scholar]
- MR imaging of the traumatic triangular fibrocartilaginous complex tear. Quant Imaging Med Surg. 2017;7:443-60.
- [CrossRef] [Google Scholar]
- Evaluation and diagnosis of wrist pain: A case-based approach. Am Fam Physician. 2013;87:568-73.
- [Google Scholar]
- Ulnar-sided wrist pain in the athlete (TFCC/DRUJ/ECU) Curr Rev Musculoskelet Med. 2017;10:53-61.
- [CrossRef] [Google Scholar]
- Biomechanical study of the extensor carpi ulnaris as a dynamic wrist stabilizer. J Hand Surg. 2012;37:2456-61.
- [CrossRef] [Google Scholar]
- Incidental signal changes in the extensor carpi ulnaris on MRI. Hand (NY). 2015;10:750-5.
- [CrossRef] [Google Scholar]
- Intrinsic ligament and triangular fibrocartilage complex (TFCC) tears of the wrist: Comparison of isovolumetric 3D-THRIVE sequence MR arthrography and conventional MR image at 3 T. Magn Reson Imaging. 2013;31:221-6.
- [CrossRef] [Google Scholar]
- Extensor carpi ulnaris injuries in tennis players: A study of 28 cases. Br J Sports Med. 2006;40:424-9.
- [CrossRef] [Google Scholar]
- Steroid injection for stenosing tenosynovitis of the extensor carpi ulnaris. J Hand Surg Eur Vol. 2019;44:425-7.
- [CrossRef] [Google Scholar]
- PRP treatment efficacy for tendinopathy: A review of basic science studies. BioMed Res Int. 2016;2016:9103792.
- [CrossRef] [Google Scholar]




