
Translate this page into:
Giant Melon seed Bodies in Painless Shoulder Swelling

*Corresponding author: Ankur Goyal, Department of Radiodiagnosis, All India Institute of Medical Sciences, New Delhi, India. ankurgoyalaiims@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Singh R, Goyal A, Srivastava DN, Gautam D. Giant Melon seed Bodies in Painless Shoulder Swelling. Indian J Musculoskelet Radiol 2021;3(1):57-9.
Abstract
Melon seed bodies are a non-specific manifestation of chronic synovial inflammation associated with various arthritides such as tubercular, rheumatoid, and seronegative arthritis. Characteristic magnetic resonance imaging (MRI) appearance of these bodies differentiates them from other differential diagnoses (such as synovial chondromatosis and pigmented villonodular synovitis). Ultrasonography and MRI, in combination with clinical and laboratory details, can suggest the possible etiology. Medical management of the underlying cause, along with arthroscopic removal of pathognomonic bodies, is the preferred treatment.
Keywords
Melon seed bodies
Subacromial-subdeltoid bursa
Bursitis
TB
Inflammatory arthritis

INTRODUCTION
Multiple melon seed bodies are usually associated with chronic inflammatory processes involving the synovium which can be due to either infective or inflammatory etiology. These loose bodies may form within the joints, and rarely in the periarticular bursae, ligament, or tendon insertion sites.[1] Subacromial-subdeltoid bursa is a rare site of involvement and often presents with massive swelling, posing diagnostic challenges. Early diagnosis is essential for specific therapy. Radiographs, ultrasonography (USG), and magnetic resonance imaging (MRI) are commonly used imaging modalities to suggest possible diagnoses and to exclude other causes. Besides, USG can be used for image-guided fluid aspiration. We report a case of isolated subacromial/ subdeltoid bursitis with giant melon seed bodies without involving glenohumeral joint in a patient with seronegative inflammatory oligoarthritis.
CASE REPORT
A 34-year-old female presented with gradually increasing painless swelling over the left shoulder for the past 4 months with no constitutional symptoms. There was a history of pain and progressive deformity of the right wrist for the past 3 years. Antinuclear antibody was positive; however, rheumatoid factor and anti-cyclic citrullinated peptide antibodies were negative. She had been diagnosed as seronegative inflammatory oligoarthritis based on laboratory investigations and hydroxychloroquine had been prescribed for the same. Wrist symptoms were attributed to inflammatory arthritic involvement.
On physical examination, there was a 7 × 8 cm non-tender, fluctuant swelling overlying the anterior, and lateral aspect of the left shoulder. The frontal radiograph showed soft-tissue opacity lateral to the shoulder joint [Figure 1] without any erosions. USG revealed the presence of loculated fluid collection in the region of subacromial subdeltoid bursa with multiple circumscribed round isoechogenic intrabursal loose bodies with slightly hyperechogenic rim and surrounding septations [Figure 2a]. On color Doppler, the septae showed vascularity [Figure 2b]. However, no vascularity was seen in the loose bodies. MRI showed that subacromial/subdeltoid bursa was distended with fluid and multiple T2 and T1 isointense (to muscle) round loose bodies were seen, suggestive of giant melon seed bodies [Figure 3a and b]. There was no blooming on gradient-echo images [Figure 3c]. No joint effusion or synovial thickening was seen. The common imaging possibilities for this appearance were infective (likely tuberculosis) and chronic inflammatory bursitis. USG-guided fluid aspiration revealed straw-colored fluid. Microscopy showed few lymphocytes but no micro-organisms. Stains for both Gram organisms as well as acid-fast bacilli were also negative. The culture of the fluid yielded no growth. Diagnosis of inflammatory subacromial/ subdeltoid bursitis with giant melon seed bodies associated with seronegative inflammatory oligoarthritis was made. As there was no pain and restriction of movement in the shoulder, the patient opted for conservative therapy. She was then referred to rheumatology for the adjustment of disease-modifying drugs. On follow-up, there was an acceptable symptomatic improvement.
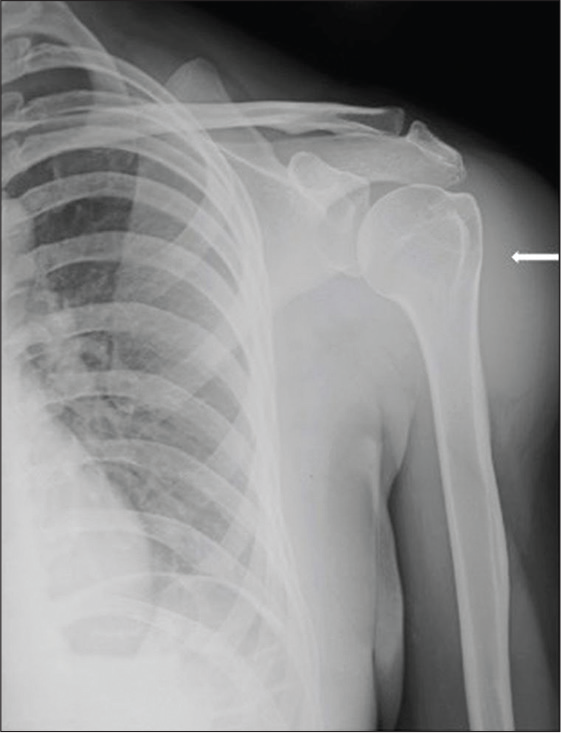
- Radiograph showed soft-tissue opacity in the left shoulder region, lateral to the joint (arrow). No erosions were seen. No widening or narrowing of joint space was seen.
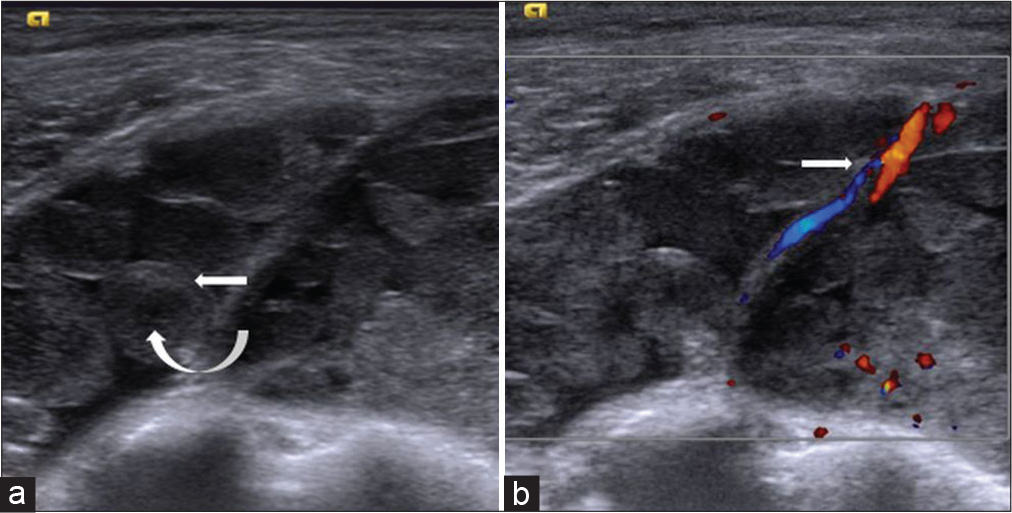
- (a) Ultrasonography showed fluid in the subacromial subdeltoid bursa with septations and multiple intrabursal round isoechoic loose bodies (curved arrow) with echogenic rims (arrow); (b) on colour Doppler, the septa showed vascularity (arrow).
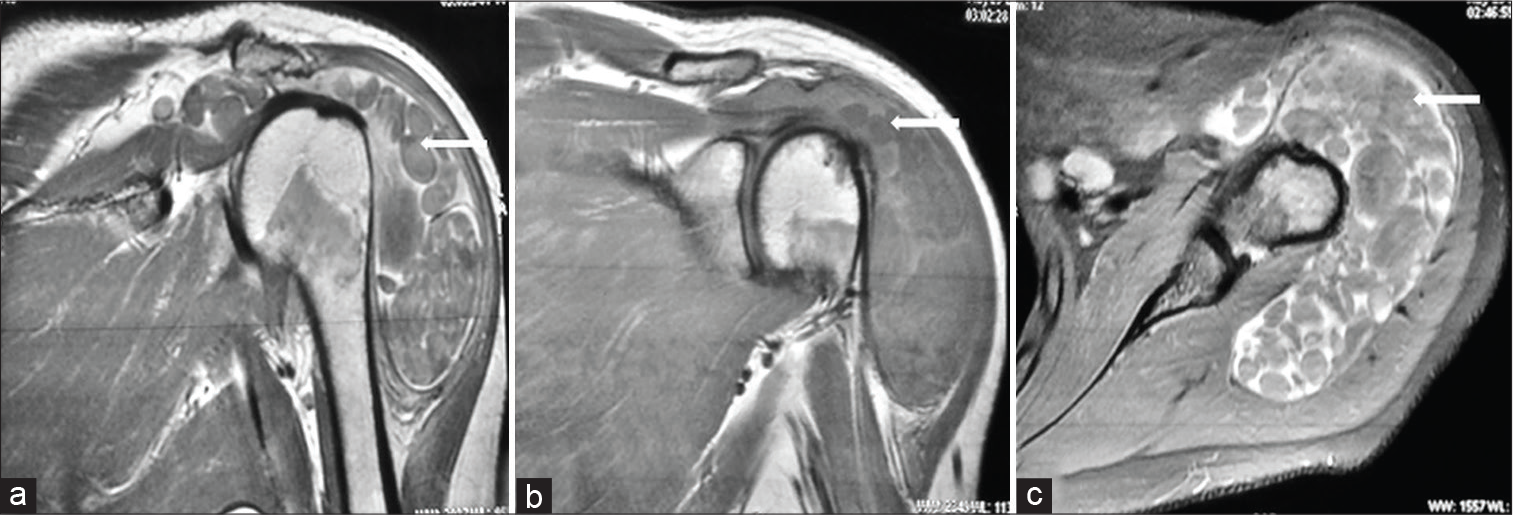
- (a) Coronal T2-weighted, (b) coronal T1– weighted, and (c) axial gradient-echo magnetic resonance imaging images show subacromial subdeltoid bursitis with multiple isointense round intrabursal loose bodies without any blooming (arrows).
DISCUSSION
Formation of the melon seed bodies is a non-specific manifestation of chronic synovial inflammation and has been reported in tuberculosis, rheumatoid arthritis, other infective arthritis, and seronegative inflammatory arthritis.[2] Its occurrence is independent of disease duration and severity. Depending on their predominant shape and appearance on synovectomy, these loose bodies may be termed as rice bodies (when longitudinal) or melon seed bodies (when round). The shape and size of loose bodies are not specific to any underlying etiology. Postulated mechanisms include synovial inflammation and microinfarcts in hypertrophic synovium, leading to detachment in the synovial cavity and subsequent fibrin deposition.[3]
The main differential diagnoses are tuberculosis, synovial chondromatosis, and pigmented villonodular synovitis (PVNS). Shoulder joint involvement with destructive erosions, periarticular osteopenia, irregular synovial thickening, and regional necrotic lymphadenopathy, along with granulomatous caseating necrosis on histopathology, suggest tuberculosis. Melon seed bodies are isointense to muscle on MRI on all sequences and isoechoic on USG.[4] Synovial chondromatosis has high T2 signal intensity in cartilaginous stage, low signal in calcific stage with blooming (on gradient-echo MR images), and isointense to the normal marrow in the ossific stage.[5] Furthermore, the calcification or ossification in these loose bodies can be evident on radiographs. PVNS demonstrates hypointense synovial thickening showing susceptibility artifact (blooming) on gradient-echo sequences due to hemosiderin deposition.
Isolated subacromial/subdeltoid bursitis with giant melon seed bodies without the involvement of glenohumeral joint is a rare cause of swelling around the shoulder joint. It has not been described in the literature previously. Medical treatment, along with arthroscopic removal of these pathognomonic bodies, is the preferred treatment in symptomatic patients.
CONCLUSION
Isolated subacromial and subdeltoid bursitis with giant melon seed bodies without the involvement of glenohumeral joint is a rare manifestation of seronegative inflammatory arthritis. Characteristic MRI imaging appearance of these bodies differentiates this morphology from other synovial diseases; however, aspiration and laboratory parameters are required to identify the etiology.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Severe sub-acromial bursitis with rice bodies in a patient with rheumatoid arthritis: A case report and review of literature. Malays Orthop J. 2018;12:52-5.
- [CrossRef] [PubMed] [Google Scholar]
- Subacromial bursitis with giant rice bodies as initial presentation of rheumatoid arthritis. J Clin Rheumatol. 2012;18:352-5.
- [CrossRef] [PubMed] [Google Scholar]
- The role of synovitis in osteoarthritis pathogenesis bone. Bone. 2012;51:249-57.
- [CrossRef] [PubMed] [Google Scholar]
- Multiple rice body formation in chronic subacromial/subdeltoid bursitis: MR appearances. Clin Radiol. 1996;51:511-4.
- [CrossRef] [Google Scholar]
- The MR appearances of synovial osteochondromatosis. J Comput Assist Tomogr. 1993;17:772-6.
- [CrossRef] [PubMed] [Google Scholar]




