
Translate this page into:
Muscle metastasis from esophageal carcinoma – Case report and review of the literature


*Corresponding author: Rajesh Botchu, Department of Musculoskeletal Radiology, Royal Orthopedic Hospital, Birmingham, United Kingdom. drbrajesh@yahoo.com
-
Received: ,
Accepted: ,
How to cite this article: Botchu R, Yousef M, Iyengar KP. Muscle metastasis from esophageal carcinoma – Case report and review of the literature. Indian J Musculoskelet Radiol. 2023;5:140-2. doi 10.25259/IJMSR_7_2023
Abstract
Muscle metastasis is rare and those from esophageal carcinoma are even rare. We report the first reported case of muscle metastasis within the vastus intermedius from squamous cell carcinoma and review the literature. Early diagnosis and awareness of the various patterns of muscle metastasis is essential to decrease morbidity.
Keywords
Metastasis
Muscle
Esophageal carcinoma

INTRODUCTION
Muscle metastases are rare with a prevalence of ranging 2–16%.[1,2] These can be synchronous or metachronous with a varied appearance on imaging. The most common primary resulting in muscle metastasis is the lung. Skeletal muscle metastasis from esophageal carcinoma is uncommon. We present the first reported case of muscle metastasis within the vastus intermedius from esophageal carcinoma and review the literature.
CASE REPORT
A 55-year-old male was referred to tertiary orthopedic oncology service with a soft-tissue lump in the right thigh. This was identified on positron emission tomography computed tomography (PET CT) as a part of the staging for esophageal carcinoma [Figure 1]. He had locally advanced squamous cell carcinoma of the lower esophagus that was being treated with chemotherapy and radiotherapy. The 2.8 cm × 2.5 cm soft-tissue lesion in the thigh was within the vastus intermedius. On magnetic resonance imaging (MRI), the lesion was isointense to muscle on T1 and hyperintense on T2 and fluid sensitive sequence (Short Tau Inversion Recovery) [Figures 2 and 3]. There was no hemorrhage or calcification within the lesion. A provisional diagnosis of Type 1 muscle metastasis or less likely soft-tissue sarcoma was considered. Ultrasound-guided biopsy was performed which confirmed the features of metastasis from esophageal squamous cell carcinoma. He was managed with radiotherapy and chemotherapy for both the primary esophageal carcinoma as well as skeletal muscle metastasis.
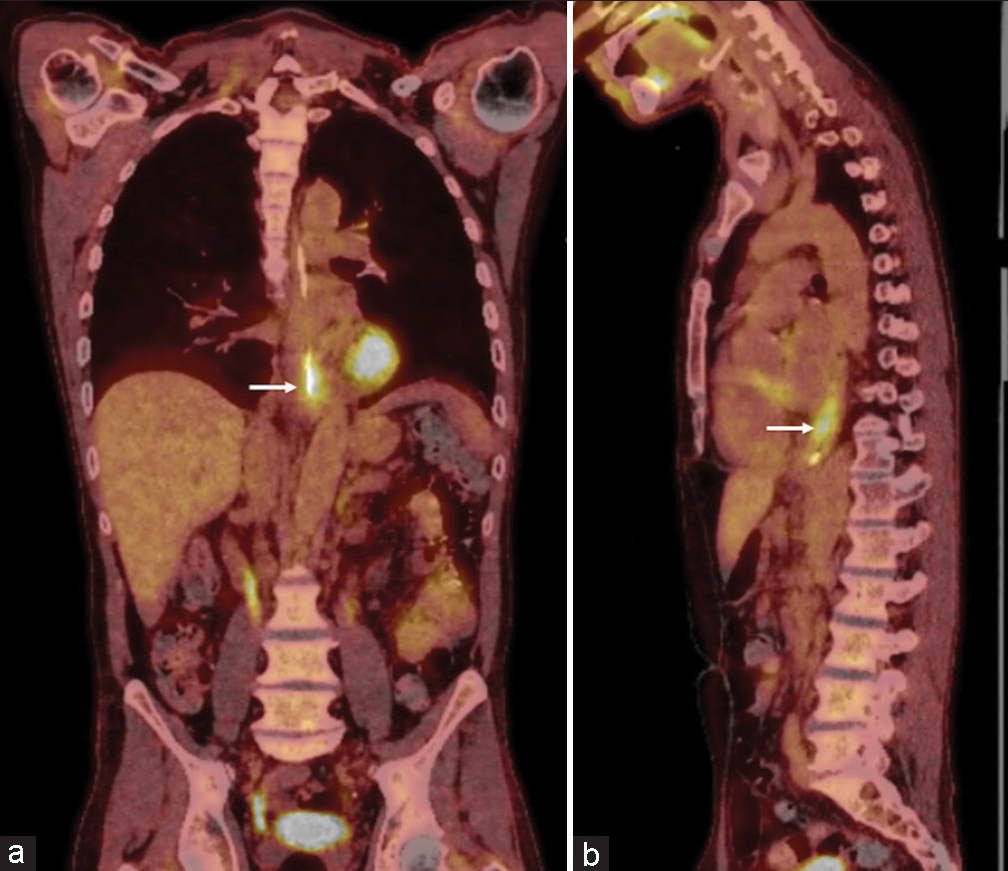
- Coronal (a) and sagittal (b) reformats of positron emission tomography computed tomography demonstrating increased uptake at the site of esophageal carcinoma of the lower esophagus (arrow).

- Axial T2 (a) and T1 (b) demonstrating lesion (arrow) within the vastus intermedius.

- Sagittal short tau inversion recovery (a) and coronal T2 (b) demonstrating metastasis within the vastus intermedius (arrow).
DISCUSSION
Muscle metastases are rare with prevalence from 1.8% to 16%.[1,2] Muscle metastasis is rare due to the anti-tumor factors present in the skeletal muscles, changes in pH, temperature, and blood pressure within the muscle.[1]
The most common primary malignancy with muscle metastasis is bronchogenic carcinoma, melanoma, renal cell carcinoma, thyroid, colon, and sarcoma. Muscle metastasis from gastrointestinal tumors is relatively uncommon.[1] Twenty one patients with muscle metastasis from esophageal carcinoma have been described with adenocarcinoma being the common type accounting for over 75%.
Esophageal cancer is the sixth most common cause of cancer death worldwide. Squamous cell carcinoma and adenocarcinoma are the most common types of esophageal carcinoma. Majority of patients with esophageal carcinoma will require palliative therapy as majority are unresectable with an aim to reduce the symptoms due to the primary tumor may be achieved using radiotherapy or stent placement.[3]
Intramuscular lesions had wide differential diagnoses and clinically, it is difficult to differentiate between them, for that reason radiology has an important role in the diagnosis and management.[1]
There are different patterns of muscle metastasis on MRI, these include peripheral enhancing metastasis, homogenous enhanced lesions and diffuse infiltrating pattern which can mimic lymphoproliferative disorders. There are two patterns which are uncommon and these can have intramuscular calcification or bleeding.[1,4]
Surov et al. described five patterns of muscle metastasis based on their imaging appearance. Metastasis with homogenous enhancement post-contrast is Type 1, Type 2 is similar to an abscess (hypointense on T1 and hyperintense on T2), and Type 3 demonstrates muscle swelling with diffuse tumor infiltration (hyperintense on T2). Metastasis with calcification (hypointense on T1 and T2) is Type 4 and Type 5 metastasis is associated with hemorrhage (hyperintense on T1).[1] The CT and imaging features would depend on the type of muscle metastasis.
The proposed mechanism of muscle metastasis is either through the arterial route, venous plexus, or intramuscular lymph nodes.[1] Distant muscle metastasis from esophageal carcinoma is extremely rare. Ludmir et al. reported Type 4 (calcifying) metastasis within the psoas muscle from a signet ring cell esophageal carcinoma.[5] These metastases are diagnosed as part of staging usually with PET CT. The average survival is 9 months after the detection of muscle metastasis.
Geukens et al. had reported a case of Type 4 metastasis within the gluteus maximus from adenocarcinoma of the esophagus.[6] The most common muscles to be involved in skeletal muscle metastasis are diaphragm, abdominal wall, glutei, deltoid, and paraspinal muscles. Sohda et al. reported a case of Type 1 muscle metastasis in adductors from adenocarcinoma of the esophagus.[7] Freer et al. reported a Type 4 ossifying metastasis within the hamstrings from adenocarcinoma of the esophagus.[8] Cincibuch et al. reported five cases of muscle metastasis from a cohort of 205 patients with esophageal carcinoma involving the quadriceps femoris, gluteus minimus, subscapularis, iliacus, and one was multiple. Two were metachronous and three were synchronous.[9] Iyengar et al. had reported a case of brachialis muscle metastasis from adenocarcinoma of the colon.[4]
The differential diagnosis of muscle lesions is myriad and would include metastasis, soft-tissue sarcoma, myositis ossificans, and muscle injury.
CONCLUSION
Muscle metastases are rare and one needs to consider this in the differential diagnosis of a muscle lesion in patients with esophageal carcinoma. Awareness of the different patterns of muscle metastasis is essential to make the diagnosis and decrease morbidity.
Ethical approval
The research/study complied with the Helsinki Declaration of 1964.
Declaration of patient consent
Patient’s consent not required as patient’s identity is not disclosed or compromised.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of Artificial Intelligence (AI)-Assisted Technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Muscle metastases: Comparison of features in different primary tumours. Cancer Imaging. 2014;14:21.
- [CrossRef] [PubMed] [Google Scholar]
- Skeletal muscle metastasis from non-small cell lung cancer. J Thorac Oncol. 2009;4:1236-41.
- [CrossRef] [PubMed] [Google Scholar]
- Palliative radiotherapy combined with stent insertion to reduce recurrent dysphagia in oesophageal cancer patients: The ROCS RCT. Health Technol Assess. 2021;25:1-144.
- [CrossRef] [Google Scholar]
- Brachialis muscle metastasis: An unusual, presenting site of metastatic adenocarcinoma of the colon. J Clin Orthop Trauma. 2022;25:101771.
- [CrossRef] [PubMed] [Google Scholar]
- Skeletal muscle metastasis from signet ring cell esophageal adenocarcinoma. Transl Gastroenterol Hepatol. 2016;1:37.
- [CrossRef] [PubMed] [Google Scholar]
- Ossifying muscle metastases from an esophageal adenocarcinoma mimicking myositis ossificans. AJR Am J Roentgenol. 2001;176:1165-6.
- [CrossRef] [PubMed] [Google Scholar]
- Primary esophageal adenocarcinoma with distant metastasis to the skeletal muscle. Int Surg. 2014;99:650-5.
- [CrossRef] [PubMed] [Google Scholar]
- Intramuscular ossifying metastasis from oesophageal carcinoma, with a pattern distinct from myositis ossificans-A case report. J Clin Orthop Trauma. 2021;24:101725.
- [CrossRef] [PubMed] [Google Scholar]
- Metastases of esophageal carcinoma to skeletal muscle: Single center experience. World J Gastroenterol. 2012;18:4962-6.
- [Google Scholar]




