
Translate this page into:
Simultaneous fracture of the neck of the femora in an adolescent

*Corresponding author: Payel Biswas, Department of Radiology, Apollo Gleneagles Hospitals Kolkata, Kolkata, West Bengal, India. itiranisarkar@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Sen SG, Datta S, Biswas P, Shah AJ. Simultaneous fracture of the neck of the femora in an adolescent. Indian J Musculoskelet Radiol. 2023;5:150-3. doi: 10.25259/IJMSR_36_2021
Abstract
A healthy adolescent boy presented with bilateral groin discomfort and pain in both lower limbs. Initial radiographs revealed fractures involving both femoral necks simultaneously, a fairly uncommon entity in the presenting age group. After a thorough clinical examination and assessment of the hormonal panel, the patient was found to have secondary hyperparathyroidism and resultant hypocalcemia, which were finally attributed to vitamin D deficiency. On normalization of serum calcium levels, both hips were stabilized post-operatively. This unique case, of simultaneous fracture of both femoral necks owing to metabolic derangements in a child, has been highlighted here.
Keywords
Bilateral
Femoral neck fracture
Radiography
Computed tomography

INTRODUCTION
Simultaneous fracture of the neck of both femora in the pediatric population is quite rare. It can occur secondary to trauma, due to nutritional causes like vitamin D deficiency, malabsorption syndromes, and even in disorders of the endocrine system like hyperparathyroidism (both primary and secondary).[1]
CASE REPORT
A 14-year-old alert and active boy presented to the emergency department accompanied by his parents, with pain in the bilateral groin and lower limbs region for 3 days. On clinical examination, the 60 kg weight boy was found to have a mild fever (temperature: 99.9°F) with mild listlessness. Sensory and motor examinations of the child appeared unremarkable. On local examination, he was having aching pain in both of his lower limbs and regional tenderness around both hip joints. He was also facing difficulty having a full range of motion in the bilateral hip joints. After a thorough history-taking, the mother as well as the child denied any history of trauma, any known tumor, overuse of any medication, use of any chronic pharmacotherapy, immunocompromised state, or any known endocrinological abnormality relevant to the clinical presentation.
Provisional clinical diagnosis was in dilemma; hence, elaborated radiological and biochemical investigations were called for.
A plain radiograph of the pelvis (anteroposterior projection) Figure 1a showed a displaced fracture of the neck of both femora in keeping with Delbet type II injury. Considering the unusual osseous presentation at this age of the child, complete blood analysis with an emphasis on metabolic blood profile was considered. Laboratory findings demonstrated deficiencies of serum calcium (5.4 mg/dL; reference range: 8–11 mg/dL), serum vitamin D3 (1.6 mg/dL; reference range: 20–40 mg/dL), and serum magnesium (1.6 mg/dL; reference range: 1.8–2.5 mg/dL) and elevated levels of serum parathyroid hormone (PTH) (162 pg/mL; reference range: 15–65 pg/mL), serum alkaline phosphatase (350 U/L; reference range: 38–126 U/L), and C-reactive protein (CRP) (44.2 mg/dL; reference range: 0.02–14.4 mg/dL). The urinary calcium–creatinine ratio appeared normal (0.02; reference range: <0.14) and ruled out hypercalcemia. Color Doppler study of both lower limbs was requested to rule out any vascular jeopardy like deep venous thrombosis or other, in a background of limb pain, mild fever, and increased serum CRP value with evidence of fracture, and the findings of Doppler ultrasound were within normal limits. For evaluation of the surrounding structures, to rule out the presence of any hematoma or foreign bodies in soft-tissue planes around both hip joints, a computed tomography (CT) scan of the pelvis region was ordered. CT scan of the pelvis, including bilateral hip joints Figure 1b, showed a displaced fracture of the neck of both femora, with no subjacent hematoma or significant soft-tissue swelling around either of the hip joints.
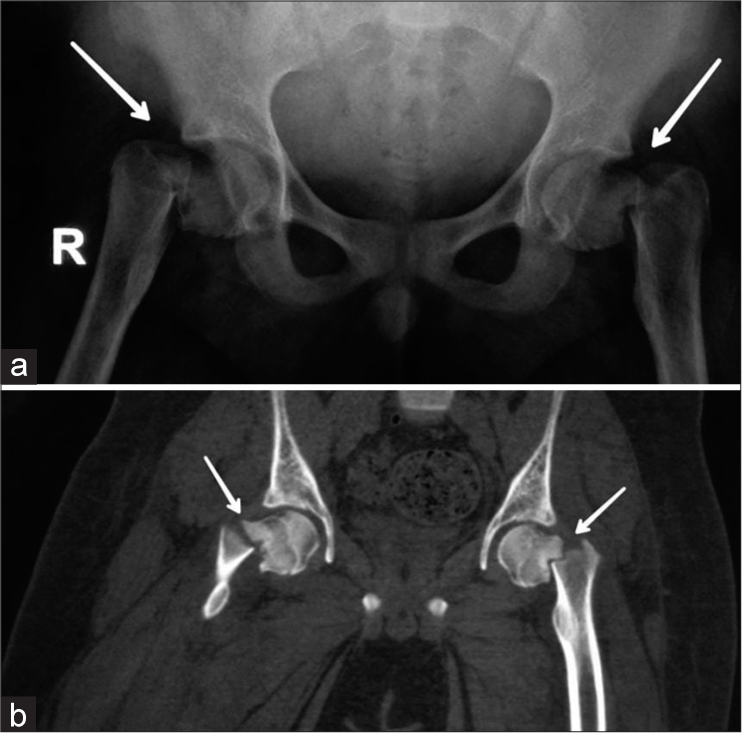
- (a) Radiograph of the pelvis with both hip joints, the frontal projection shows complete and displaced fracture of the neck of both femora (arrows), consistent with Delbet type II. (b) Computed tomography scan of the pelvis with both hip joints in coronal acquisition depicts the same findings (arrows) as in radiography.
The reduced levels of serum calcium and serum vitamin D3 with elevated levels of serum PTH, serum alkaline phosphatase, and increased CRP narrowed down the clinical diagnosis to be of metabolic origin. A skeletal survey was done; however, no obvious fracture anywhere else, and no other imaging findings of hyperparathyroidism were noted. Therefore, the final diagnosis of simultaneous fracture of the bilateral femoral neck (Delbet type II) in a background of vitamin D deficiency was made. An etiological diagnosis of secondary hyperparathyroidism was made owing to vitamin D deficiency status and raised serum parathormone.
Hypocalcemia was corrected with parenteral calcium gluconate, followed by oral calcium supplements. After normalization of serum calcium, open reduction, and internal fixation were performed for both fractures and thereby both hip joints were stabilized. An additional subtrochanteric valgus osteotomy [Figure 2]; was planned on two sittings, over 6 weeks. The postoperative period was uneventful. Oral calcium and vitamin D supplementation was given for the next 3 months. Restriction to activities like weight-bearing/lifting was advised, followed by adequate physiotherapy comprising isometric quadriceps exercises and passive range exercises of both hip joints for a couple of months. At a subsequent follow-up visit in the 9th month, the patient ambulated independently, yielding a full and painless range of movements of both hip joints.
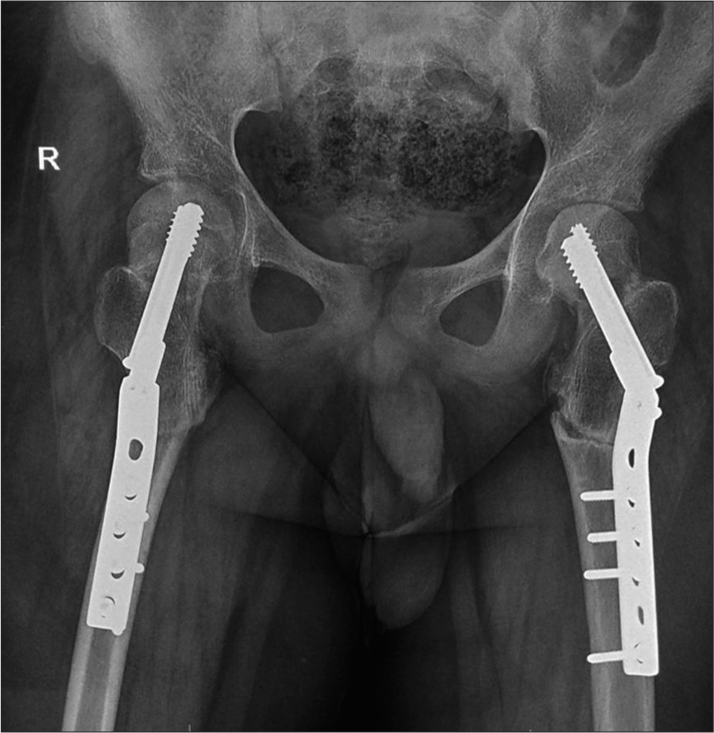
- Radiograph of the pelvis with both hip joints. Post-operative status. Fixation screws in situ stabilizing both hip joints. Joint spaces and subjacent soft-tissue shadows appear normal.
DISCUSSION
Fracture of the neck of the femur is a common type of injury in the elderly but is quite uncommon when noted bilaterally. In children, bilateral femoral neck fractures are seldom seen; the majority occur secondarily in settings of trauma, such as falls, electric shock, episodes of lightning, electroconvulsive therapy, and seizures.[1] Interestingly, insufficiency fractures also can involve the femoral neck. Although insufficiency fractures or stress fractures have been largely discussed in osteoporotic bones predominantly in the elderly population, any metabolic process that has the potential for bone weakening can be an important predisposing factor. Certain vitamin deficiencies and/or endocrine dysfunction tend to disrupt bone mineral homeostasis and can lead to these types of insufficiency fractures.
Calcium and phosphate homeostasis is crucial for normal bone function in our body, and the two major hormones responsible are the PTH and Vitamin D3 (active form). Deficiencies of Vitamin D3 decrease circulating calcium leading to defective bone calcification and bone weakness. Diseases from deficiency of PTH or its overproduction (hypo- or hyperparathyroidism) have reciprocal effects on calcium and phosphate homeostasis. Secondary hyperparathyroidism, induced by any acquired condition, causes serum calcium to fall. This decreases the circulating calcium again with defective calcification of the bones, and thereby bone weakness and softening.[2]
In children and adolescents, Vitamin D deficiency and associated hypocalcemia are not uncommon, be it from inadequate exposure to sunlight (might be a possibility in our case that could be aggravated in COVID-19 pandemic settings, for being indoors) or a dietary deficiency.[3,4] However, the whole constellation is usually subclinical and majorly asymptomatic, thus under investigated and hence under reported.[1,5] The child in our case did not have any obvious radiological evidence of osteoporosis (although we could not perform a DEXA scan for this patient as it is not done in our institute and the patient was unable to get it done from outside). The background risk factors for osteoporosis in our case were only noted in the blood level, i.e., newly diagnosed hyperparathyroidism and hypovitaminosis D.
Plain radiography is the first line investigation for suspected femoral neck fractures with sensitivity being above 90%. Other advanced imaging modalities such as magnetic resonance imaging (MRI) and multidetector computed tomography (MDCT) are also recommended by standard authorities as the next-line investigations with a sensitivity of MRI being almost 100%. Recent studies revealed that the sensitivity of thin-slice MDCT was as high as MRI in the evaluation of fractured neck femur cases; therefore, we recommend a CT scan as the 2nd line investigation in these cases due to cost-effectiveness and easier availability than MRI.[6]
Classification of fractured neck femur is important for the assessment of the prognosis as well as treatment purposes. The risk of non-union and osteonecrosis or avascular necrosis (AVN) of the femoral head is fairly high if left untreated, especially in children due to tenuous blood supply and osseous anatomy.[7] The risk of AVN in children may be as high as 92% in these fractures.[8] The Delbet classification is helpful in assessing the risk of developing AVN of the femoral head and to guide management, either conservative or operative, and is particularly useful in cases of children. Intracapsular fractures of the femoral neck are the most prone to developing AVN. Type II in the Delbet classification is a transcervical fracture, and it is the most common type of pediatric femoral neck fracture, as in our case. More importantly, the development of osteonecrosis is also very common in type II fractures.
Ideally, a fractured neck of the femur should be addressed surgically and operated on within 24 hours.[9] In our case, the late presentation of the patient and further delay for stabilization have led the management to be staged in two different settings. Pauwels angle (basis of biomechanical classification) and the interval between fracture and surgery are the most crucial factors for the management of fracture of the neck of the femur.[10] Pauwels angle calculates the angle between the fracture line of the distal fragment and the horizontal line to determine the shearing stress and compressive force. Subtrochanteric osteotomy helps obtain a favorable Pauwels angle and is the standard practice in the delayed presentation to allay non-union, as performed in our case too, and resulted in an expected favorable outcome for the child.
CONCLUSION
In this interesting case, simultaneous fracture of both femoral necks resulted from the metabolic derangements only as evidenced by extensive investigations. Hence, the need for undertaking a complete metabolic and radiographic bone profile in an apparently healthy, asymptomatic adolescent individual presenting with this kind of extremely rare bilateral osseous presentation cannot be overemphasized.
Acknowledgment
We thank Dr. Usha Goenka, MD, Head of the Department of Radiology and Imaging, and Dr. Soumya Paik, MS, Department of Orthopedics [Apollo Gleneagles Hospital, Kolkata, West Bengal, India], for contributory advice.
Ethical approval
The research/study complied with the Helsinki Declaration of 1964.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript, and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Simultaneous bilateral neck of femur fractures in an adolescent secondary to hypocalcaemic seizure. J Pediatr Orthop B. 2019;28:491-4.
- [CrossRef] [PubMed] [Google Scholar]
- Evaluation, treatment, and prevention of vitamin D deficiency: An Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2011;96:1911-30.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence of Vitamin D deficiency among healthy adolescents. Arch Pediatr Adolesc Med. 2004;158:531-7.
- [CrossRef] [PubMed] [Google Scholar]
- COVID-19: The endocrine opportunity in a pandemic. Minerva Endocrinol. 2020;45:204-27.
- [CrossRef] [PubMed] [Google Scholar]
- Simultaneous bilateral femoral neck fractures: Case report. Swiss Surg. 2001;7:222-4.
- [CrossRef] [PubMed] [Google Scholar]
- The validity of investigating occult hip fractures using multidetector CT. Br J Radiol. 2016;89:1060.
- [CrossRef] [PubMed] [Google Scholar]
- Femoral neck fractures in children: A review. Indian J Orthop. 2018;52:501-6.
- [CrossRef] [PubMed] [Google Scholar]
- Risk factors for avascular necrosis after femoral neck fractures in children: 25 Cincinnati cases and meta-analysis of 360 cases. J Orthop Trauma. 2006;20:323-9.
- [CrossRef] [PubMed] [Google Scholar]
- Managements of femoral neck fracture in the young patient. A Critical analysis review. World J Orthop. 2014;5:204-7.
- [CrossRef] [PubMed] [Google Scholar]
- An update on the Pauwels classification. J Orthop Surg Res. 2016;11:161.
- [CrossRef] [PubMed] [Google Scholar]




