
Translate this page into:
The Importance of Avoiding Satisfaction of Search Bias in a Case of Concurrent Calcaneonavicular Coalition and Osteoid Osteoma

*Corresponding author: Rajesh Botchu, Department of Musculoskeletal Radiology, Royal Orthopedic Hospital, Birmingham, West Midlands, United Kingdom. drbrajesh@yahoo.com
-
Received: ,
Accepted: ,
How to cite this article: Hurley P, Panchal H, Kho J, Botchu R. The Importance of Avoiding Satisfaction of Search Bias in a Case of Concurrent Calcaneonavicular Coalition and Osteoid Osteoma. Indian J Musculoskelet Radiol 2020;2(2):133-5.
Abstract
We report a rare case of concurrent calcaneonavicular osseous coalition and osteoid osteoma of the navicular. While each pathology is relatively common, the combination of the two in one foot is rare and as such can present a unique challenge to imaging interpretation. This case reinforces the importance of the concept of “satisfaction of search.”
Keywords
Osteoid osteoma
Coalition
Satisfaction of search

INTRODUCTION
Hind foot pain is a common complaint to primary care.[1] The majority of causes of hind foot pain can be localized to one of six anatomical regions: The plantar fascia, calcaneus, tarsal tunnel, tendons, bursae, and plantar fat pad.[2] Hind foot pain is typically considered an issue of the elderly, however up to 10% of individuals below the age of 45 will report hind foot pain.[3] There are myriad causes of hind foot pain in young adults. These include tarsal coalition, which can be fibrous, cartilaginous, or osseous, and benign tumors, for example, osteoid osteomas (OOs) which are not especially uncommon in the foot, but are relatively rare in the navicular.[4] We report a case of a 17-year-old male with concurrent osseous calcaneo navicular coalition and OO of the navicular.
CASE REPORT
A 17-year-old male presented with a 8-month history of insidious hind foot pain. There was no history of trauma and his medical history was unremarkable. He was investigated with magnetic resonance imaging (MRI) and computed tomography (CT) of the foot.
MRI depicted osseous edema in the navicular, calcaneum, cuboid, and lateral cuneiform. The anterior process of the calcaneum was elongated and in continuity with the navicular, in keeping with an osseous calcaneonavicular coalition. In addition, MRI demonstrated a 8 mm lesion in the navicular adjacent to the site of osseous calcaneonavicular coalition [Figure 1]. The articular cartilage of calcaneocuboid, talonavicular, and subtalar joints was preserved without any joint effusion.
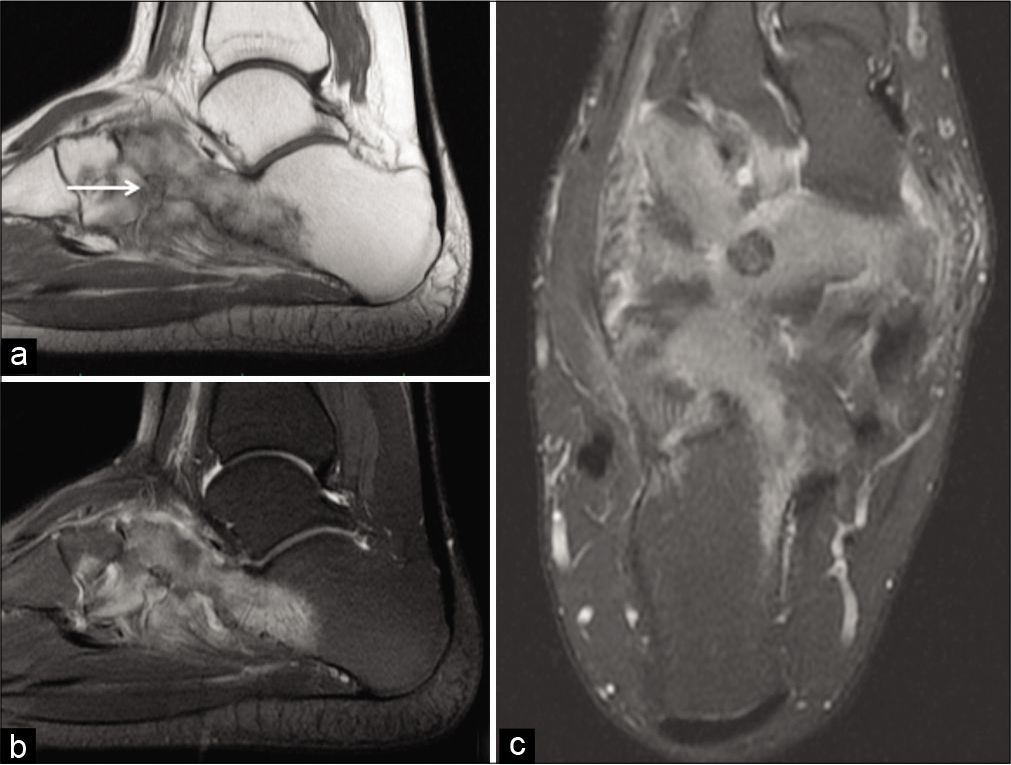
- Sagittal T1 (a), proton density fat-suppressed (PDFS) (b), axial PDFS (c) showing osseous calcaneonavicular coalition with osteoid osteoma of navicular (arrow) with marked osseous edema of the calcaneum, navicular, cuboid, and lateral cuneiform.
CT was performed to further investigate the navicular lesion identified on MRI. This showed 8 mm lucent lesion with central focus of calcification confirming the presence of an OO in the navicular [Figure 2]. The OO of the navicular was referred for radiofrequency ablation; however, this was not performed due to patient’s financial circumstances.
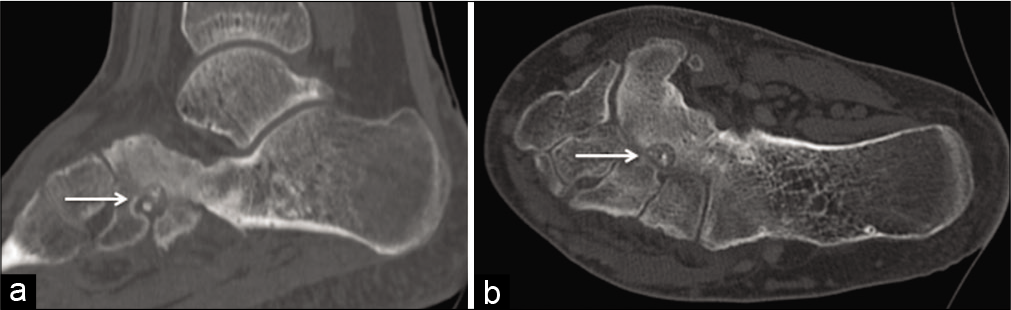
- Sagittal (a) and axial (b) computed tomography showing an osteoid osteoma (arrow) of the navicular with calcaneonavicular coalition.
DISCUSSION
Tarsal coalition refers to complete or partial union between bones of the mid and hindfoot. Tarsal coalitions are developmental malformations of the foot and are not degenerative in etiology. Approximately 5% of the population will develop tarsal coalition, with the condition typically presenting in adolescence.[5] Two main forms of tarsal coalition comprise 90% of all cases, namely, talocalcaneal and calcaneonavicular coalition.[6] Tarsal coalition can be subdivided according to the nature of the tissue connecting the bones of the midfoot and of the hind foot. These are osseous, cartilaginous, and fibrous. Tarsal coalitions typically present with foot pain and stiffness. Tarsal coalitions may be managed conservatively, but definitive treatment requires surgery to correct the underlying abnormality. Surgical options include osteotomy or coalition removal.
OOs are benign neoplasms, which typically develop in the cortex of the long bones of the lower limbs. They may also be identified in other regions of the body such as the spine, or, in <5% of cases, in the bones of the foot. It has been reported that the highest incidence of OOs can be seen between the ages 4 and 25 and that males are twice as likely to be affected as females.[4] OOs typically cause constant and progressive pain that is worse at night. Pronounced symptomatic relief with NSAID analgesia is typical. Definitive treatment is by radio frequency ablation or surgical resection with curettage.
In our case, there was concurrent OO of navicular with osseous calcaneonavicular coalition. To the best of the authors’ knowledge, the co-occurrence of both pathologies in the same region of the foot has not been previously described in the literature. However, as calcaneonavicular coalition in particular is not uncommon, the co-occurrence of both pathologies in this case may be coincidental, rather than reflecting an underlying association.
This case highlights the importance of the concept of “satisfaction of search” in interpreting radiological studies.[7] This term refers to the observed phenomenon, whereby the identification of one radiographic sign impacts on the ability to detect others. Satisfaction of search bias can be considered as an error of cognition and more specifically of perception, the most common error of perception being non-identification errors. This is particularly relevant in this case because the clinical history of pain and the MRI findings of osseous edema could have been attributed to the calcaneonavicular coalition alone, should the more subtle OO been missed. To overcome, this bias Rogers[8] and Graber et al.[9] recommend adopting a systematic approach to interpreting imaging. Kok et al.[10] discuss this in greater detail by theorizing on the importance of analytic (systematically reviewing entire images) as opposed to non-analytic reasoning (pattern recognition and rapid diagnosis).
CONCLUSION
This case acts as an excellent example, whereby two relatively uncommon conditions presenting in a similar manner have been diagnosed simultaneously. While under normal conditions a diagnosis of either in isolation would not present a challenge to an experienced orthopedic surgeon or radiologist, the combination of the two may easily be missed. It is essential for image readers to be aware of potential shortcomings due to satisfaction of search bias and to work systematically to evaluate images for potential concurrent diagnoses.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
Dr. Rajesh Botchu is on the Advisory Board of this journal. He does not have any competing interest.
References
- Epidemiology of posterior heel pain in the general population: Cross-sectional findings from the clinical assessment study of the foot. Arthritis Care Res (Hoboken). 2015;67:996-1003.
- [CrossRef] [PubMed] [Google Scholar]
- Painful heel: MR imaging findings. Radiographics. 2000;20:333-52.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence and correlates of foot pain in a population-based study: The North West Adelaide health study. J Foot Ankle Res. 2008;1:2.
- [CrossRef] [PubMed] [Google Scholar]
- Skeletal benign bone-forming lesions. Eur J Radiol. 1998;27(Suppl 1):S91-7.
- [CrossRef] [Google Scholar]
- Congenital tarsal coalition: Multimodality evaluation with emphasis on CT and MR imaging. Radiographics. 2000;20:321-32. quiz 526-7, 532
- [CrossRef] [PubMed] [Google Scholar]
- MDCT of the abdomen: Missed diagnoses due to satisfaction of search. AJR Am J Roentgenol. 2010;195:W314-6.
- [CrossRef] [PubMed] [Google Scholar]
- Bringing diagnosis into the quality and safety equations. JAMA. 2012;308:1211-2.
- [CrossRef] [PubMed] [Google Scholar]
- Systematic viewing in radiology: Seeing more, missing less? Adv Health Sci Educ Theory Pract. 2016;21:189-205.
- [CrossRef] [PubMed] [Google Scholar]




