
Translate this page into:
Sonographic and MRI presentation of geyser sign in rotator cuff tears

*Corresponding author: Amandeep Singh, Department of Radiodiagnosis and Imaging, SGRD Institute of Medical Sciences and Research, Amritsar, Punjab, India. dr.amancs@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Singh A, Devgan A, Khatana J, Singh G. Sonographic and MRI presentation of geyser sign in rotator cuff tears. Indian J Musculoskelet Radiol 2021;3:103-5.
Abstract
Limited cases of rotator cuff tears with acromioclavicular (AC) degeneration in association with cystic swelling or ganglion cyst have been described till date. The “geyser radiographic sign” was originally described by Craig in 1984. Its significance was to document a tear in the articular capsule of the AC joint in the setting of a chronic full-thickness tear of the rotator cuff, which gave the appearance of a geyser arising from the subacromial bursa as radiographic contrast tracked through the AC joint to project superiorly from the shoulder. An 82-year-old male presented with pain on rest in the left shoulder and with difficulty in overhead abduction from last few months. MRI showed near complete full-thickness tear of supraspinatus tendon with retraction of the tendon and reduced bulk of the supraspinatus muscle with associated superior subluxation of humerus with AC arthropathic changes causing ganglion cyst and incidental finding of superior labrum anterior and posterior tear. AC cysts are further divided into Type 1 and Type 2. Repeated aspirations of these masses are not advised, as they often recur and repeated attempts at aspiration may lead to formation of a draining fistula. MRI geyser sign is highly suggestive of a benign process, which suggests underlying rotator cuff pathology.
Keywords
Geyser sign
MRI shoulder
AC Joint
Chronic rotator cuff tears

INTRODUCTION
The rotator cuff is comprised of supraspinatus, infraspinatus, subscapularis, and teres minor muscles and tendons. The supraspinatus and infraspinatus tendons spread-out and intermingle, at the distal aspect of the rotator cuff, forming an uninterrupted insertion on the middle facet of the humeral greater tuberosity.[1] Originally described in 1984, the “geyser radiographic sign” by Craig on a shoulder arthrogram was represented as seepage of radiographic contrast from the glenohumeral joint into the subdeltoid bursa. It is implied to represent a tear in the articular capsule of the acromioclavicular (AC) joint, as radiographic contrast tracks through the AC joint. It projects superiorly from the shoulder, appearance of a geyser arising from the subacromial bursa is seen commonly in setting of a chronic full-thickness tear of the rotator cuff. Limited cases of rotator cuff tears with AC degeneration in association with cystic swelling or ganglion cyst have been described till date. Classic radiographic signs that were once used to document injury during arthrography have been translated into analogous findings on MRI which is now considered the mainstay in orthopedic imaging for shoulder.[2]
CLINICAL AND IMAGING FINDINGS
An 82-year-old male presented in the orthopedics department with pain on rest in the left shoulder with difficulty in overhead abduction from the past few months. On physical examination, there was evidence of a well-defined fluctuant swelling over the AC joint which was associated with pain as well. Due to clinical doubt of degenerative arthritis of the AC joint and subcutaneous plane involvement, ultrasound evaluation was done on Philips Affiniti 50 G using MSK probe (5–18 MHz) and MRI correlation of the shoulder was conducted on a 1.5 T MR scanner. On ultrasound, a well-defined mass lesion, appearing heterogeneously hypoechoic with multiple septae noted within it was seen superior and medial to the AC joint [Figure 1]. On color Doppler flow imaging, there was no significant vascularity. Furthermore, a hypoechoic defect within the tendon of supraspinatus was noted as a concavity in the normal convex contour [Figure 2]. MRI showed near complete full-thickness tear of supraspinatus tendon with retraction of the tendon and reduced bulk of the supraspinatus muscle (Goutallier classification – Stage IV). There was associated superior subluxation of humerus with AC arthropathic changes. A multiloculated cystic collection appearing hyperintense on T2-weighted and fat-saturated T2-weighted images and few internal septations was seen in the subcutaneous plane and subdeltoid bursa displaying the geyser sign [Figures 3 and 4]. Hyperintensities were also noted in the glenoid labrum extending from 12 to 2O’ clock position on fat-saturated proton-density images suggestive of superior labrum anterior and posterior tear type IIa.
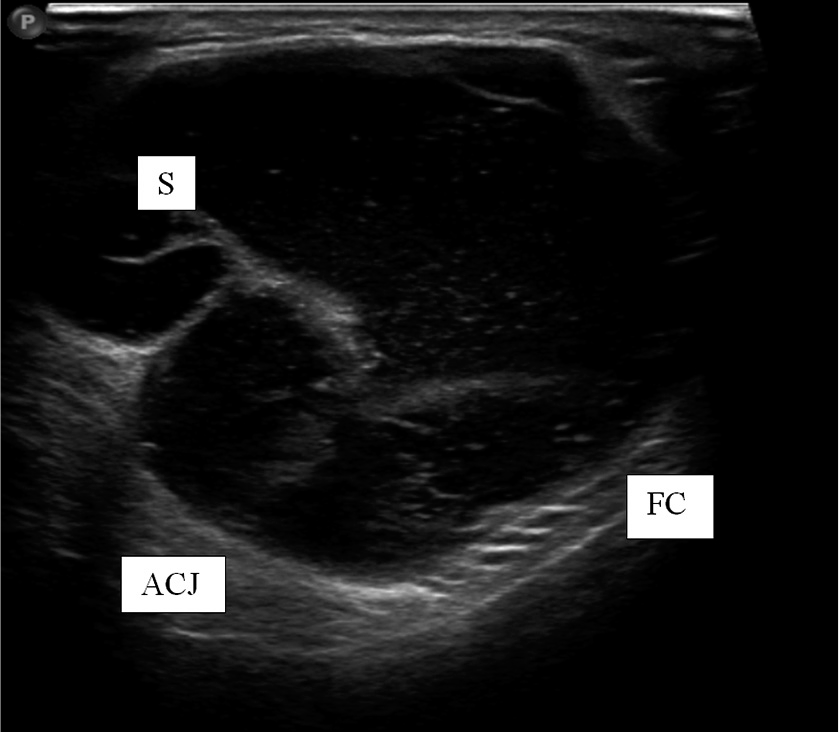
- Supraspinatus tear with geyser sign. S: Septa, FC: Fibrous capsule, ACJ: Acromioclavicular joint.

- Supraspinatus tendon tear with retraction. DM: Deltoid muscle. Residual fibers of near complete tear are seen.
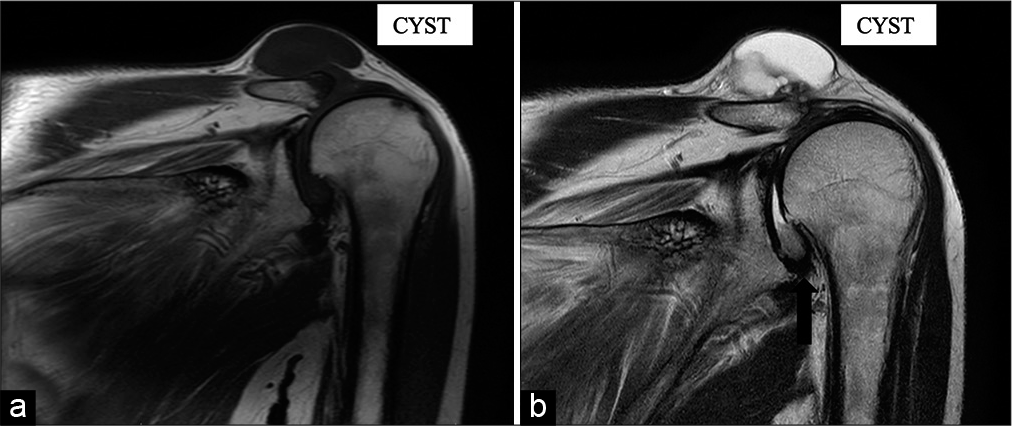
- Coronal T1SE (a) and T2TSE (b) images demonstrate a large lobulated cystic lesion overlying the acromioclavicular joint and proximal migration of humerus (black arrow).
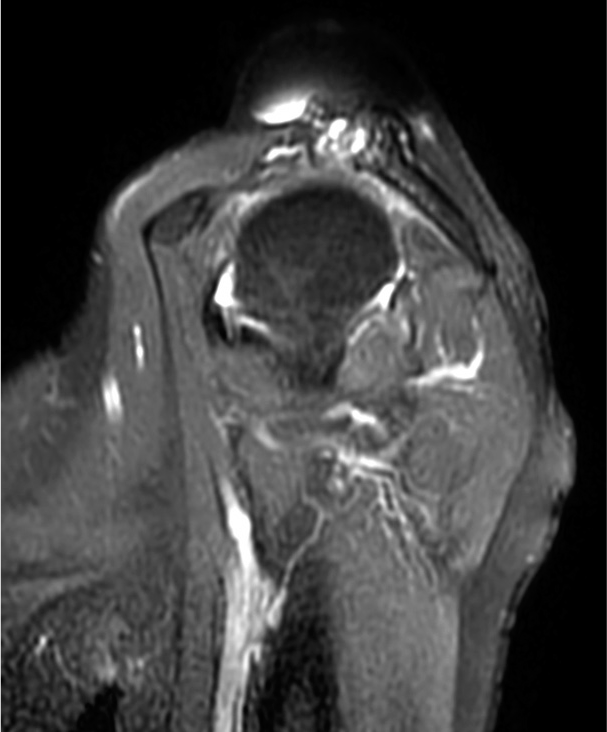
- Sagittal FSPD image reveals near complete tear of the supraspinatus and conjoint tendons with superior subluxation of the humeral head. Degenerative changes in the form of subarticular cysts of the humeral head (white arrow) and synovitis involving the acromioclavicular joint.
DISCUSSION
AC joint cysts are a rare clinical disorder. The cysts are further divided into Type 1 and Type 2. Type 1 cyst is limited to the AC joint seen intact within rotator cuff in superficial location. Mechanical instability of the humeral head due to immeasurable or traumatic tears of the rotator cuff can cause overproduction of synovial fluid and weakening of the inferior AC capsule. In type 2 cysts, a “geyser” of fluid can form between the glenohumeral and the AC joint.[3] The definite pathogenesis of AC joint type 2 cyst is not entirely comprehended. There is a presumed theory when the synovial fluid in the glenohumeral joint escapes through full-thickness supraspinatus tendon tear into the subacromial bursa, it then decompresses across an osteoarthritic AC joint [Figure 5]. Cystic mass formation may occur due to expansion, outpouching, and probably rupture of the superior capsule of AC joint due to amplified intra-articular fluid pressure.[4] Ganglion cyst, lipoma, juxta-articular cysts, synovial cyst, tumor, or an infectious process can be reserved as radiological differentials.[5]
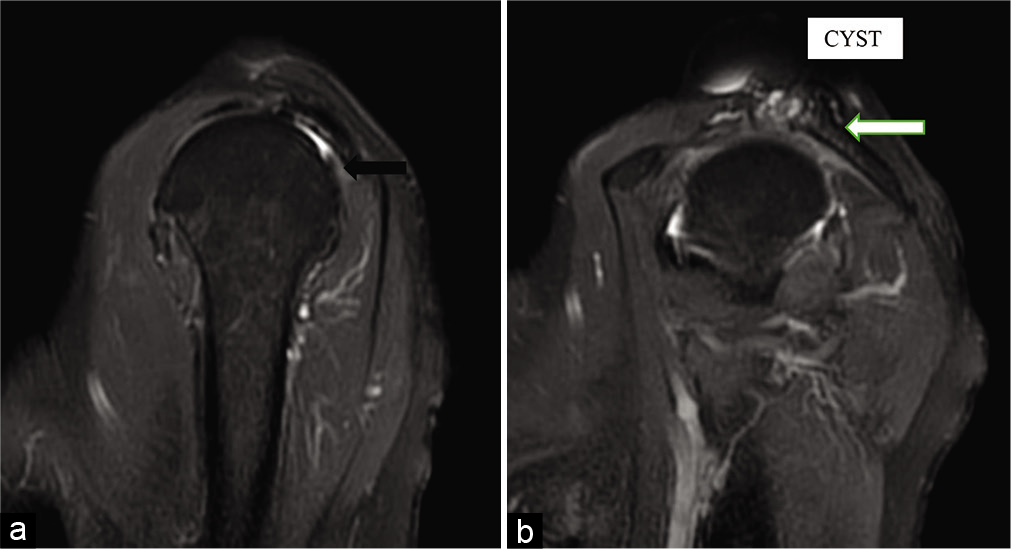
- Sagittal PD FATSAT images (a and b) reveal near-complete tear of the supraspinatus and conjoint tendons (black arrow). Chronic arthropathy (white arrow) and large lobulated cystic lesion overlying the acromioclavicular joint.
In general, repeated aspirations of these masses are not advised as they recur frequently and repeated efforts at aspiration may cause a draining fistula formation, requiring surgical attention.
Excisional AC joint arthroplasty ought to be performed with sufficient resection of the base of the cyst, to remove the oneway “pinch-valve effect” and to prevent future recurrence, when the rotator cuff defect is irreparable.[6] In this case, the patient was managed with surgical excision and postoperative period was uneventful.
Geyser sign provides very valuable information about the integrity of the supraspinatus tendon tear. This sign usually occurs due to large, full-thickness, and chronic rotator cuff tear. MRI geyser sign is extremely indicative of a benign process, suggesting a primary rotator cuff pathology.[7]
CONCLUSION
AC joint cyst is a rare mechanical complication of a degenerative and massive rotator cuff tear in elderly patients, potentially misdiagnosed as a tumor. In assessment of a shoulder lump for the presence of malignancy, the validation of the geyser sign indicates a benign process. Imaging, especially MRI, should be performed to exclude malignancy and make an accurate diagnosis, identifying the “Geyser sign.”
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent form.
Financial support and sponsorship
Nil.
Conflicts of interest
There is no conflict of interest.
References
- Acromioclavicular joint cyst formation. Clin Anat. 2010;23:145-52.
- [CrossRef] [PubMed] [Google Scholar]
- The geyser sign and torn rotator cuff: Clinical significance and pathomechanics. Clin Orthop. 1984;19:213-15.
- [CrossRef] [Google Scholar]
- MR imaging of rotator cuff injury: What the clinician needs to know. RadioGraphics. 2006;26:1045-65.
- [CrossRef] [PubMed] [Google Scholar]
- Clinics in diagnostic imaging 151. Acromioclavicular joint geyser sign with chronic full-thickness supraspinatus tendon (SST) tear. Singapore Med J. 2014;55:53-6.
- [CrossRef] [PubMed] [Google Scholar]
- MR Geyser Sign in chronic rotator cuff tears. Med J Armed Forces India. 2018;74:304-6.
- [CrossRef] [PubMed] [Google Scholar]
- The MRI geyser sign: Acromioclavicular joint cysts in the setting of a chronic rotator cuff tear. Am J Orthop (Belle Mead NJ). 2011;40:118-21.
- [Google Scholar]
- Sonographic presentation of the geyser sign. Case Rep Med Hindawi; 2019. 2019:1-3.
- [CrossRef] [PubMed] [Google Scholar]




