
Translate this page into:
Ring-shaped meniscus with absent anterior cruciate ligament: A rare association with review of the literature


*Corresponding author: Rajesh Botchu, Department of Musculoskeletal Radiology, Royal Orthopedic Hospital, Birmingham, United Kingdom. drrajeshb@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Rahij H, Hassan M, Ariyaratne S, Botchu R. Ring-shaped meniscus with absent anterior cruciate ligament: A rare association with the review of the literature. Indian J Musculoskelet Radiol. 2024;6:49-52. doi: 10.25259/IJMSR_62_2023
Abstract
A spectrum of congenital and anatomical variants of a lateral meniscus can be encountered, including discoid meniscus, ring meniscus, double-layered meniscus, hypoplastic meniscus, and accessory meniscus in the knee joint. These can be associated with a plethora of abnormalities predominantly involving the anterior cruciate ligament (ACL) of the knee. Morphological abnormalities of the menisci can present in unusual ways, leading to clinical dilemmas and providing a diagnostic challenge. We report a case of a 26-year-old male presenting with a rare combination of ring meniscus, a hypoplastic ACL, and an oblique inter-meniscal ligament to raise awareness of the condition. Pertinent literature is also reviewed.
Keywords
Meniscus
Ring-shaped meniscus
Anterior cruciate ligament
Magnetic resonance imaging

INTRODUCTION
The menisci in the knee joint are fibrocartilaginous discs, primarily made of type I collagen and perform roles of deepening the articular surface, broadening the contact area, transmitting force, and mechanoproperiroception function in the knee joint.[1] Injuries and abnormalities of menisci represent a common cause of knee pain and orthopedic intervention. However, several morphological and anatomical variations of the lateral meniscus of the knee joint exist, such as the discoid meniscus, hypoplastic meniscus, double-layered meniscus, and ring-shaped meniscus.[2] Hence, it is crucial that a focused clinical history, examination, and complementary imaging are undertaken in patients presenting with knee pain to lead to appropriate patient management.
Unlike the typical crescent-shaped meniscus, its ring-shaped variant of the lateral meniscus is characterized by the presence of an intermeniscal bridge connecting the anterior and posterior horns, resulting in the formation of a complete ring-shaped meniscus.[3] A ring meniscus is a rare anatomical variant among all other meniscal morphological abnormalities.[4,5] Typically, patients with ring-shaped meniscus remain asymptomatic unless it is accompanied by other concurrent abnormalities or malformations of the knee. These include hypoplasia or absence of anterior cruciate ligament (ACL), accessory meniscus, and double-layered meniscus.[6,7] However, a ring meniscus can mimic a bucket handle tear or incomplete discoid meniscus.[8,9] Magnetic resonance imaging (MRI) can play a crucial role in the effective diagnosis of this condition and target patient management.[10]
Herein, we present the case of a 26-year-old male patient who presented with the chief complaint of his knee “giving way” and was found to have a ring-shaped meniscus alongside a hypoplastic ACL on MRI and review the current literature on this rare combination. It will highlight awareness of the condition and help in situations of clinical dilemma following a common knee presentation.
CASE REPORT
A 26-year-old male footballer presented to the sports injury clinic with recurrent episodes of instability while running and changing direction. He had little confidence in his right knee and experienced severe pain when the knee gave way. He had not experienced symptoms of locking or recurrent swelling of the knee. There was no history of direct or indirect trauma. There was no other relevant past medical or surgical history.
On examination, the overall knee alignment was satisfactory, with no deformity. His gait was satisfactory. The right knee revealed no obvious swelling or peri-articular wasting. There was lateral joint line tenderness with normal tracking of the patella. The collateral ligaments appeared intact when assessed with valgus and varus stress tests, and McMurray’s test was negative. However, he demonstrated sagittal plane instability on stress testing (anterior drawer and Lachman tests positive). The knee revealed a full range of active and passive motion from 0 to 120° of flexion. The ipsilateral hip examination was normal, and there was no evidence of generalized joint hypermobility. The posterolateral corner clinically appeared intact. The neurovascular examination revealed no abnormality.
A screening weight-bearing plain radiograph demonstrated no osseous abnormality. A subsequent MRI of the right knee was performed, with routine proton-density (PD)-weighted and PD fat-suppressed sequences obtained in three planes in a 3 Tesla MRI scanner. This revealed a ring-shaped lateral meniscus with a “classic mirror sign” (the inner component of the meniscus mirrored the classic lateral meniscal triangular configuration). The inner fragment of the ring meniscus was within the medial part of the lateral tibiofemoral joint [Figures 1 and 2]. There was no tear of the ring-shaped lateral meniscus. The medial meniscus was of normal configuration apart from an absent posterior root. There was a hypertrophied lateral oblique intermeniscal ligament attaching to the anterior horn of the lateral meniscus and the posterior horn of the medial meniscus [Figures 1 and 2], and the ACL was absent. The tibial eminence was also hypoplastic with absent tibial spines. The medial collateral ligament, iliotibial band, posterolateral corner, popliteus, and extensor mechanism were normal. The lateral collateral ligament was intact but lax. No features of patellofemoral mal-tracking were noted.
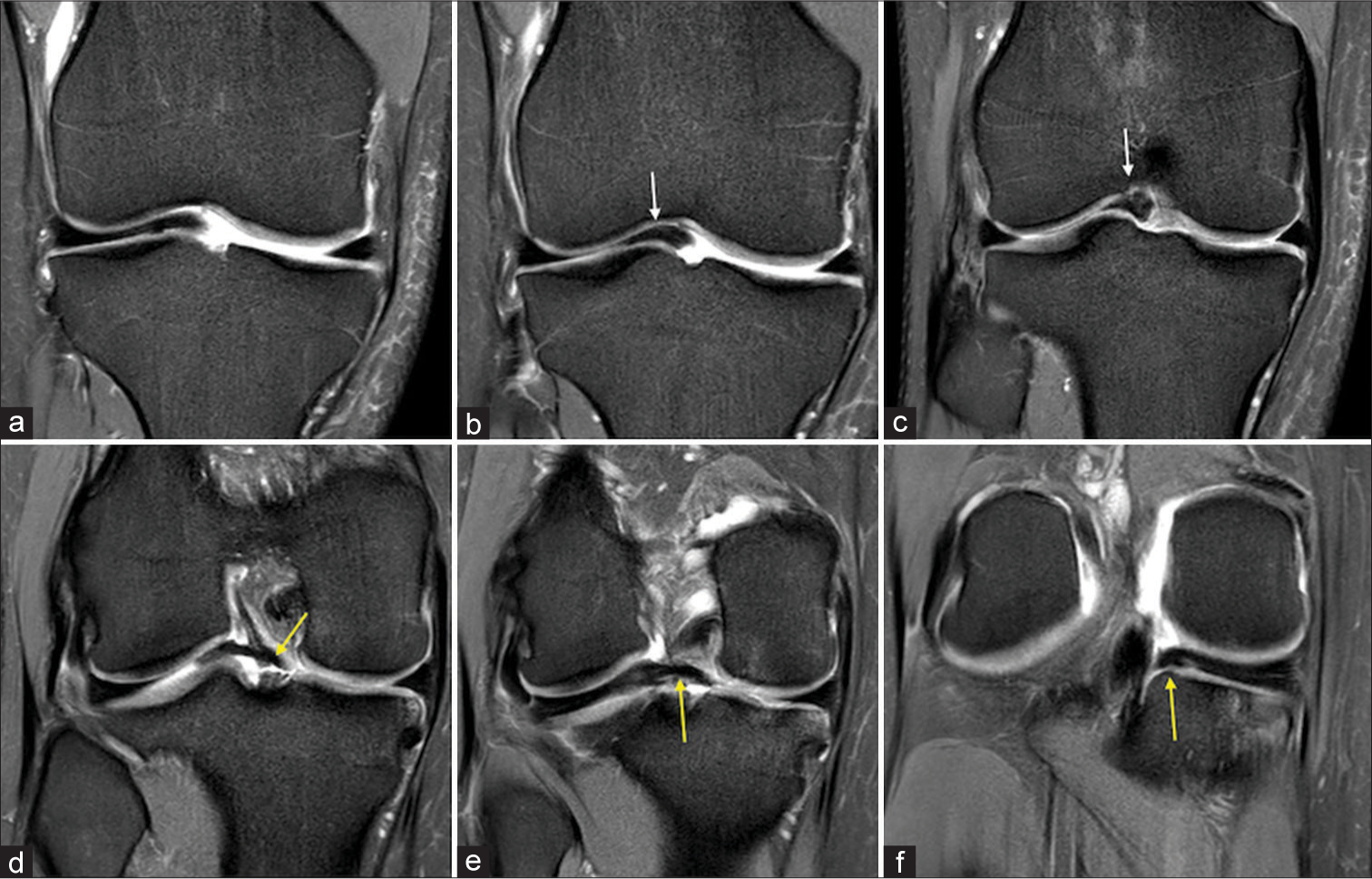
- (a-f) Coronal proton-density fat-suppressed sequences of the right knee from anterior to posterior (a-f) demonstrating a ring-shaped lateral meniscus (white arrows) and a hypertrophied lateral oblique intermeniscal ligament (yellow arrows). Also note the absence of the anterior cruciate ligament and hypoplastic tibial eminence.
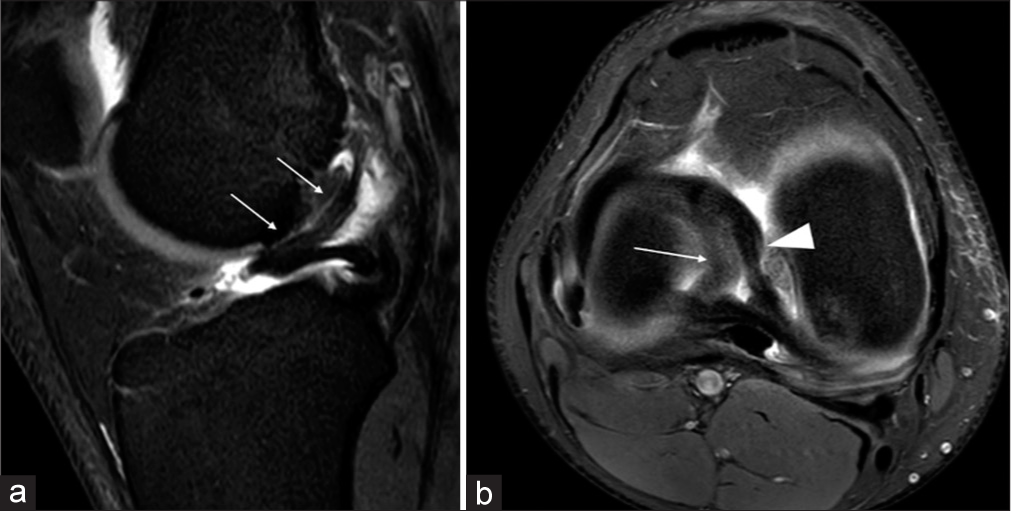
- (a and b) Sagittal proton-density fat-suppressed (PDFS) (a) and axial PDFS (b) sequences of the right knee. The hypertrophied lateral oblique inter meniscal ligament is well demonstrated in the sagittal image (a, white arrows). Axial image (b) demonstrating the attachment of the lateral oblique intermeniscal ligament to the anterior horn of the lateral meniscus and posterior horn of the medial meniscus (white arrowhead) and the ring-shaped morphology of the lateral meniscus (white arrow).
The need for a knee arthroscopy was discussed with the patient to confirm the MRI findings and the possibility of confirming the morphological variant. However, the patient declined and was advised to follow a Patient-Initiated Follow-Up (PIFU) regime (PIFU-patient able to request an appointment if the symptoms are problematic) set up in our hospital. In the interim, he was advised analgesia and recommended a supervised physiotherapy regime at his sports club.
DISCUSSION
The ring meniscus, although a rare abnormality, is increasingly being recognized as a definite clinical entity.[3-5] Its incidence is thought to be between 0.9%.[3] This was first described involving the medial meniscus in 1930 by Watson-Jones.[7] It is important to differentiate a discoid lateral meniscus from a ring-shaped meniscus. Whereas a discoid meniscus generally appears as an isolated abnormality finding on an MRI scan of the knee, the ring meniscus may appear in combination with other ligamentous and meniscal abnormalities. The possibility of other abnormalities such as ACL deficiency, absence of posterior horn of medial meniscus, and abnormal orientation of the intermeniscal ligament should be borne in mind when a ring meniscus is noted.[5]
Ring meniscus is usually asymptomatic.[5] Unlike a discoid meniscus or bucket handle tear of the meniscus, the inner portion of the ring meniscus is not mobile.[5] Ring meniscus can be associated with the accessory meniscus, which arises from the anterolateral part of the lateral tibial plateau and is inserted on the inner component of the ring meniscus, with two such cases reported in literature.[5] Double-layered meniscus is a rare variant with an incidence of 0.05–0.09% that can be associated with ring meniscus. These can be the connected variant or the separated variant. The latter involves the connection of the periphery of the meniscus with the ring meniscus. The association of ring meniscus with ACL agenesis was first described on autopsy in 1975.[6] Noble described the first case of ring meniscus with hypoplasia of ACL in 1975.[11]
The cause of this combination of abnormalities remains unclear. We believe that it is either triggered by a genetic abnormality or may be developmental due to “abnormal” biomechanical triggers. It is suggested that the cause of discoid meniscus is congenital, and histological examination may show a disorder of collagen fibers and greater thickness.[12,13]
Due to the paucity of data in the literature regarding the ring meniscus, the natural course and long-term prognosis of a ring-shaped meniscus seem uncertain. However, due to the complex nature of the pathologies, such as the absence of a part of the meniscus and ACL deficiency, it may be assumed that such knees may develop early degeneration.[12,13]
The involvement of a musculoskeletal radiologist would aid in the identification of multiple and subtle associated pathology. This “syndrome” of pathologies with ring meniscus may trigger more complex treatments, such as ACL reconstruction and meniscal root stabilization, rather than a simple arthroscopic partial meniscectomy.[13] A clear distinction should be made between the bucket handle tears and the “ring meniscus.” Iqbal et al. highlighted the salient features, such as the position of the inner component of the ring meniscus and the “central bow sign”, which aid in the diagnosis of the ring meniscus.[3] A ring meniscus also typically has smooth and symmetrical margins on both the lateral and medial sides (the “classic mirror sign”) with smooth tapering of the inner aspect of the “ring,” as opposed to the irregular appearance seen with bucket handle type tears [Table 1].
| Bucket handle meniscal tear | Ring meniscus | |
|---|---|---|
| Incidence | Relatively common | Rare |
| Symptoms | Symptomatic and can present with locked knee | Asymptomatic unless associated with a meniscal tear |
| Ends of meniscus | Truncated | Smooth and tapering |
| Medial part of the meniscus |
In the intercondylar notch |
Medial part of meniscus- intermeniscal bridge adjacent to the intercondylar notch and lying between the articular cartilage of femur and tibia |
Learning points
Ring meniscus may coexist with a congenitally deficient meniscus
Careful interpretation of the MRI scan by a musculoskeletal radiologist is essential in all cases with suspected ring meniscus
A clear history focused on understanding the presentation symptom that is, instability, locking or both, with or without a history of trauma, may help in establishing the diagnosis
Early identification of the ring meniscus and ACL deficiency may help in planning treatment better.
CONCLUSION
If patients develop recurrent instability of the knee without any history of trauma, they should be investigated further with an MRI Scan. A musculoskeletal radiologist should get involved early, and the possibility of a “syndrome of congenital ligamentous and meniscal pathology”, as outlined above, should be explored.
Ethical approval
The Institutional Review Board approval is not required.
Declaration of patient consent
Patient’s consent is not required as the patient’s identity is not disclosed or compromised.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript, and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- MR-arthrography: Anatomic variant from link between lateral meniscus and anterior and posterior cruciate ligaments. A case report and review of the literature. Radiol Case Rep. 2021;16:3012-5.
- [CrossRef] [PubMed] [Google Scholar]
- The ring-shaped meniscus: A case series demonstrating the variation of imaging appearances on MRI. Skeletal Radiol. 2020;49:281-9.
- [CrossRef] [PubMed] [Google Scholar]
- "Ring-shaped" meniscus and accompanying intermeniscal bridge meniscus: A rare combined variant resembling a bucket-handle tear. Skeletal Radiol. 2024;53:805-9.
- [CrossRef] [PubMed] [Google Scholar]
- Ring-shaped lateral meniscus combined with an accessory meniscus: A rare anatomical variant. J Orthop Surg (Hong Kong). 2020;28:2309499019893059.
- [CrossRef] [PubMed] [Google Scholar]
- Ring-shaped lateral meniscus with the hypoplasic anterior cruciate ligament. Skeletal Radiol. 2015;44:1813-8.
- [CrossRef] [PubMed] [Google Scholar]
- Ring meniscus mistaken for incomplete discoid meniscus: A case report and review of literature. Knee Surg Sports Traumatol Arthrosc. 2010;18:543-5.
- [CrossRef] [PubMed] [Google Scholar]
- Symptomatic ring-shaped lateral meniscus. Arthroscopy. 2000;16:852-4.
- [CrossRef] [PubMed] [Google Scholar]
- Symptomatic ring-shaped lateral meniscus. MRI findings. BMJ Case Rep. 2011;2011:bcr1020114914.
- [CrossRef] [PubMed] [Google Scholar]
- Congenital absence of the anterior cruciate ligament associated with a ring meniscus. J Bone Joint Surg Am. 1975;57:1165-6.
- [CrossRef] [PubMed] [Google Scholar]
- Absence congénitale du ligament croisé antérieur. A propos de 8 cas [Congenital absence of the anterior cruciate ligament: Eight cases in the same family] Rev Chir Orthop Reparatrice Appar Mot. 2005;91:642-8.
- [CrossRef] [PubMed] [Google Scholar]




