
Translate this page into:
Isolated distal plantaris tendon rupture – An unusual cause of posterior calf pain

*Corresponding author: Rajesh Botchu, Department of Musculoskeletal Radiology, Royal Orthopedic Hospital, Birmingham, United Kingdom. drrajeshb@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Botchu R, Amissah-Arthur J, Giakoumis M, Beale D. Isolated distal plantaris tendon rupture – An unusual cause of posterior calf pain. Indian J Musculoskelet Radiol. 2024;6:61-4. doi: 10.25259/IJMSR_47_2023
Abstract
Plantaris muscle is a vestigial plantar flexor of the ankle running across the back of the leg as a part of the triceps surae muscle complex. Although injuries to the plantaris are uncommonly described, its rupture can mimic more clinically relevant conditions such as deep vein thrombosis or Achilles tendon tears. We present an interesting case of distal plantaris tendon rupture in a 19-year-old elite-international 400m sprinter mimicking Achilles tendon/soleus muscle injury and describe the clinico-radiological features, including the management strategy of this unusual injury.
Keywords
Tendon injuries
Achilles tendon
Plantaris
Tennis leg
Ankle joint
Magnetic resonance imaging

INTRODUCTION
The Plantaris muscle is a vestigial muscle in human beings, as Homo sapiens adopted a bipedal, biphasic upright gait. It is a part of the triceps surae muscle complex, along with the gastrocnemius and soleus muscles.[1] The plantaris muscle is of questionable physiological importance and is absent in 7–10% of the population.[2] It is reported to be a weak plantar flexor of the ankle and weak knee joint flexor but is considered to have a proprioceptive function due to the presence of a high density of muscle spindles.[3] Isolated reports of proximal muscle, mid-calf, and distal plantaris tendon rupture have been described in the literature, highlighting the need for vigilance to identify and manage this often-missed injury.[4-6]
Applied anatomy of plantaris muscle
The plantaris muscle has a long, thin muscle belly and a long, thin tendon with different mechanical properties to the Achilles tendon. The plantaris arises from the lateral supracondylar line of the distal femur, just superior and medial to the lateral head of the gastrocnemius muscle, and from the oblique popliteal ligament on the posterior aspect of the knee joint [Figure 1]. The plantaris muscle belly lies deep to the lateral head of the gastrocnemius muscle, varies in size from 7–13 cm and the thin tendon courses distally in medial-inferior direction. The tendon courses between the two heads of the gastrocnemius muscle and the myotendinous junction are situated at the level of origin of the soleus muscle from the tibia in the proximal leg. Further, the plantaris tendon courses obliquely and medially, lying between the soleus muscle and the medial head of the gastrocnemius muscle. Distally, it runs along the medial border of the Achilles tendon toward its insertion on the posterior surface of the calcaneus, just anteromedial to the Achilles tendon. The insertion can be variable as an independent insertion or in a complex pattern.[7] The plantaris tendon insertion may merge with the Achilles tendon as a conjoined tendon insertion into the calcaneus.[8] An intact plantaris tendon in the presence of Achilles tendon rupture may still allow active plantar flexion of the ankle and present a clinical conundrum.[9]
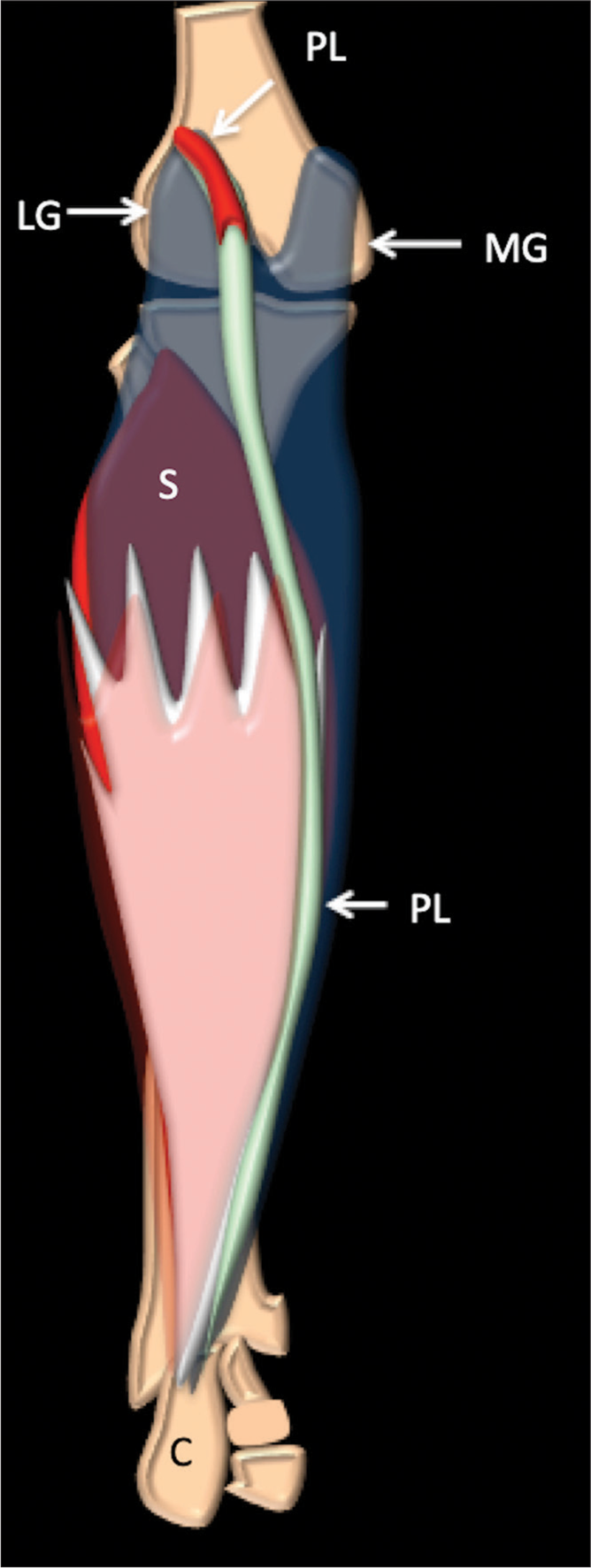
- Schematic anatomy plantaris muscle, tendon, and relationships in the back of the calf. (MG: Medial gastrocnemius, LG: Lateral gastrocnemius, S: Soleus , C- calcaneum, and PL- plantaris).
CASE REPORT
A 19-year-old elite international 400m sprinter noticed an acute onset of pain in the back of his left calf as he was sprinting around the bend during a 400m race. He was otherwise fit and well with no comorbidities. The pain progressed over the next 2–3 days and he started to limp slightly but was still able to compete in two finals. Clinical examination revealed tenderness along the medial part of the Achilles tendon at approximately 5 cm proximal to the insertion. Thompson test to evaluate Achilles tendon rupture was negative, and symmetrical spontaneous hindfoot plantarflexion in the prone position was possible.
Magnetic resonance imaging (MRI) was undertaken, which confirmed rupture of the distal part of the plantaris tendon with mild edema about 5 cm proximal to the calcaneus, with an intact Achilles tendon [Figures 2 and 3]. The popliteal arteries and veins were normal. There was no evidence of strain or tear at the medial head of the gastrocnemius or the rest of the triceps surae muscle complex. No fluid collection was noted in the calf. A clinico-radiological diagnosis of distal plantaris tendon rupture was made. The patient was treated conservatively.
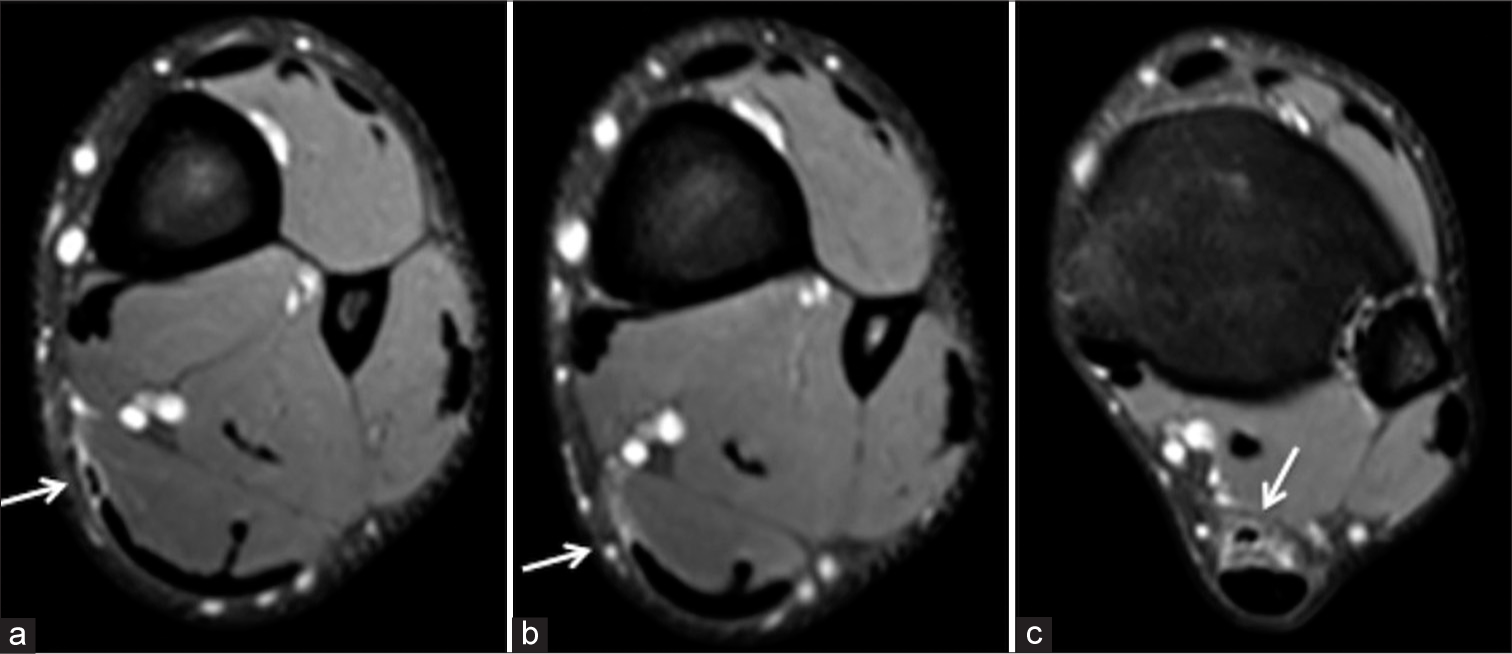
- (a-c) Proton density fat-saturated (PDFS) axials at the levels shown - demonstrate fluid in relation to the (a,c) distal plantaris (arrow) and (b) full thickness tear of plantaris (arrow).
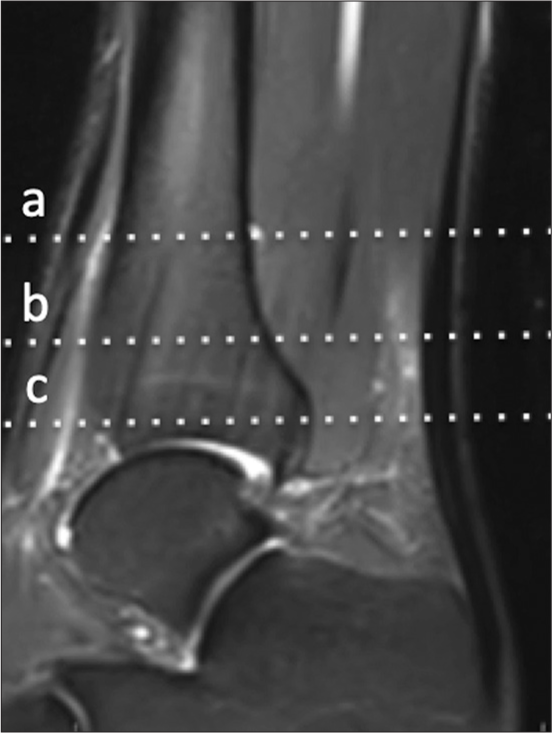
- (a-c) Proton density fat-saturated (PDFS) sagittal showing levels at which axials of figures a-c have been obtained.
Differential diagnosis
With the presentation feature and mechanism of injury, gastroc-soleus tear or Achilles tendon rupture should be ruled out with clinico-radiological evaluation. Deep venous thrombosis is another possibility.
DISCUSSION
Plantaris muscle, as a vestigial muscle, does not have a biomechanically significant function in the lower extremity. However, as a part of the triceps surae muscle complex and like the gastrocnemius muscles, the plantaris muscle traverses two joints, which may make it more susceptible to injury and ruptures.[9]
Due to the nature of its course at the back of the calf, plantaris tendon ruptures may mimic other common, clinically significant injuries or conditions, such as deep venous thrombosis in the leg.[4]
The most common mechanism of plantaris rupture is sudden dorsiflexion of the ankle with the knee in full extension in an actively contracting triceps surae muscle complex. This seems to be the mode of plantaris rupture in our patient. The injury most likely occurred during sprinting around a bend where more tension would be placed on the plantaris tendon due to its muscle course as the foot would be in a position of dorsiflexion, eversion and the knee moving into extension. The sudden, sharp pain in the calf is typical of the commonly described “tennis leg” and may imitate a strain of medial gastrocnemius or Achilles tendon rupture at the musculotendinous junction. The term “tennis leg” was first described by Powell as a clinical entity in 1883.[10] Although “tennis leg” is classically caused by a rupture of the plantaris muscle, the term is also used frequently to describe a strain of the medial head of the gastrocnemius muscle or the soleus muscle since these are more common.[11] The term “tennis leg” may be a misnomer since other reported cases in the literature of plantaris tendon ruptures have been due to a fall, playing football or a sudden push-off during sprinting, as seen in our presentation.[4,5,12] It is interesting to note that the athlete was able to complete his race and complete three further races over the next three days, winning two finals.
A focused history, mechanism of injury, and clinical assessment are crucial to distinguish between plantaris tendon rupture and other common calf muscle injuries. This is particularly important from the management point of view since the gastrocnemius or soleus injuries are generally more severe and require longer to heal. A dedicated rehabilitation regimen and splinting technique may be required. A positive Thompson test is a good clinical sign to diagnose Achilles tendon rupture in such situations.
The injuries in the calf and triceps surae muscle complex may be impossible to differentiate clinically and, herein, lays the significance of complementary imaging such as ultrasound (US) of the calf and MRI. US may be able to detect fluid in the muscle planes and hypoechoic changes around area of the rupture. A Doppler US will show patency of veins. Hence, MRI is the investigation of choice in such injuries. MRI provides a non-invasive modality of assessment and can accurately distinguish between these entities in the calf. MRI can highlight the site of the tear, localize the retraction of the muscle, and more significantly be able to detect associated injuries such as strain of the medial head of gastrocnemius muscle or the Achilles tendon.[13,14] MRI is thus useful in differentiating between other clinically significant causes of calf pain, such as deep venous thrombosis, medial gastrocnemius or soleus muscle tears, compartment syndrome, or Achilles tendon rupture. This is crucial for appropriate treatment of the patient’s injury.
Once the diagnosis of isolated rupture of plantaris is clinico-radiologically confirmed, the treatment is essentially conservative since plantaris rupture does not result in any significant loss of function.[4] This keeps in line with what was observed in our case study. An uneventful recovery is expected with traditional non-operative treatment of physiotherapy, analgesia and a gradual muscle strengthening and rehabilitation regimen.[5]
CONCLUSION
This case report highlights that injuries to the distal plantaris tendon can be an uncommon cause of calf pain. It can present with a confusing clinical picture and mimic other common, clinically significant injuries such as an Achilles tendon rupture, or medial gastrocnemius/soleus tear or deep venous thrombosis, depending on the site of the plantaris muscle/tendon tear. A high index of clinical suspicion, complementary MRI and gradual muscle strengthening, and rehabilitation regimen can help to manage plantaris tendon ruptures in an effective manner.
Ethical approval
The Institutional Review Board approval is not required.
Declaration of patient consent
Patient’s consent is not required as patients identity is not disclosed or compromised.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Anatomy of the triceps surae: A pictorial essay. Foot Ankle Clin. 2014;19:603-35.
- [CrossRef] [PubMed] [Google Scholar]
- The plantaris tendon graft: An ultrasound study. J Hand Surg Am. 1991;16:708-11.
- [CrossRef] [PubMed] [Google Scholar]
- The plantaris muscle: Anatomy, injury, imaging, and treatment. J Can Chiropr Assoc. 2007;51:158-65.
- [Google Scholar]
- Plantaris rupture: Why is it important? BMJ Case Rep. 2013;2013:bcr2012007840.
- [CrossRef] [PubMed] [Google Scholar]
- Isolated rupture of the distal plantaris muscle. J Foot Ankle Surg. 2018;57:995-6.
- [CrossRef] [PubMed] [Google Scholar]
- Surgically documented rupture of the plantaris muscle: A case report and literature review. Foot Ankle Int. 1997;18:522-3.
- [CrossRef] [PubMed] [Google Scholar]
- A highly complex variant of the plantaris tendon insertion and its potential clinical relevance. Anat Sci Int. 2020;95:553-8.
- [CrossRef] [PubMed] [Google Scholar]
- It is NOT the gastrocnemius, soleus, or Achilles … What could it be? A plantaris muscle injury. Curr Sports Med Rep. 2015;14:84-5.
- [CrossRef] [PubMed] [Google Scholar]
- Tennis leg: Clinical US study of 141 patients and anatomic investigation of four cadavers with MR imaging and US. Radiology. 2002;224:112-9.
- [CrossRef] [PubMed] [Google Scholar]
- Diagnosis and follow-up US evaluation of ruptures of the medial head of the gastrocnemius ("tennis leg") Korean J Radiol. 2006;7:193-8.
- [CrossRef] [PubMed] [Google Scholar]
- Rupture of plantaris muscle-a mimic: MRI findings. J Clin Imaging Sci. 2012;2:19.
- [CrossRef] [PubMed] [Google Scholar]
- Imaging of plantaris muscle rupture. Clin Imaging. 1992;16:55-8.
- [CrossRef] [PubMed] [Google Scholar]
- Tennis leg: Gastrocnemius injury is a far more common cause than plantaris rupture. Radiol Case Rep. 2016;12:120-3.
- [CrossRef] [PubMed] [Google Scholar]




