
Translate this page into:
Soft-tissue tumor of myoepithelial origin in leg with secondary bone changes: A rare case report

*Corresponding author: Preksha Mukeshbhai Mer, Department of Radiodiagnosis, B. J. Medical College, Gujarat Cancer Research Institute, Ahmedabad, Gujarat, India. preksha98765@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Mer PM, Parikh KA. Soft-tissue tumor of myoepithelial origin in leg with secondary bone changes: A rare case report. Indian J Musculoskelet Radiol. 2024;6:116-9. doi: 10.25259/IJMSR_20_2024
Abstract
Myoepithelial tumors in skin and soft tissue are uncommon, but have been increasingly characterized over the past decades. They equally affect men and women of all age groups. Lesions are more frequent in extremities and limb girdles. Due to presence of varied architectural and cytological features both within a lesion and between different tumors, immunohistochemistry may be required to diagnose these tumors. We report a rare case of myoepithelial tumor of soft tissue of lower extremity with secondary bone changes on radiographs, as well as magnetic resonance imaging and histopathological correlation. The tumor was initially noticed as a painless, deep soft-tissue mass in the left lower limb; thereafter, the patient started complaining about chronic left lower limb radicular pain. A core needle biopsy was then performed, which discloses nests of ovoid to plasmacytoid cells having monomorphic round nuclei, inconspicuous nucleoli, and clear cytoplasm. Immunohistochemically, the tumor cells were positive for AE1, P40, CK 5/6, and vimentin markers.
Keywords
Myoepithelial tumor
Magnetic resonance imaging
Fluid-fluid levels
Bone remodeling

INTRODUCTION
Myoepithelial carcinomas of salivary glands are much more common and well-recognized in the salivary glands, but they rarely appear in soft tissue and bone. However, morphological characteristics of myoepithelial carcinoma in soft tissue are similar to those found in salivary gland myoepithelial carcinoma. They can occur in any age group but are present typically before the 4th decade with majority of lesions involving extremities.[1-3] They are primarily encountered in structures with glandular or ductal tissues although more frequently found in bone, soft tissue, as well as cutaneous tissues.[1,3] Myoepithelial tumors constitute a very heterogenous morphologic and immunophenotypic features. Although a benign histological pattern is identified in roughly 50% of salivary gland myoepithelial tumors, the great majority of myoepithelial tumors that develop in soft tissue are malignant.[1,3] Soft-tissue myoepithelial carcinomas are equally prevalent in both genders. In this report, we represent a 40-year male presented with a case of myoepithelial tumor of lower extremity.
CASE REPORT
A 40-year-old male patient presented with a slowly growing, palpable mass in his left calf region. The patient had chronic radicular left leg pain and numbness in the left foot. His past medical history included poorly controlled hypertension. On examination, there was mildly tender, smooth-contoured, and firm mass in left calf region. On radiographs, there was large soft-tissue fullness, which caused pressure erosion and reactive sclerosis over adjoining aspects of tibia and fibula. There was anterior bowing of tibia with large craniocaudally oriented lytic-sclerotic areas as a result of disorganized bone growth and coarsened trabeculae involving anterior cortex of left tibia [Figure 1]. On magnetic resonance imaging (MRI), the mass exhibited a heterogeneous solid appearance with multiple cystic spaces showing fluid-fluid levels within [Figure 2]. There was heterogeneous post-contrast enhancement [Figure 3]. The lesions showed a lobulated dumbbell-like side-to-side extension across interosseous membrane. The anterior tibial cortex showed bony expansion with disorganized new bone formation, without evident tumor-like enhancing areas or marrow signal alterations. On microscopic examination, there were epithelioid cells with moderate amount of cytoplasm and monomorphic round nuclei, with some of the cells showing nucleoli [Figure 4]. On immunohistochemistry (IHC), the tumor cells were positive for AE1, P40, CK 5/6, and vimentin markers [Figure 5], but negative for SATB-2, S-100, and actin. Finally, a diagnosis of soft-tissue myoepithelial tumor was offered based on the above histologic features.

- (a) Anteroposterior (b) Lateral radiograph of left leg showing large soft-tissue fullness, which causes pressure erosion and reactive sclerosis over adjoining aspects of tibia and fibula. There is anterior bowing of tibia with large craniocaudally oriented lytic-sclerotic area as a result of disorganized bone growth and coarsened trabeculae involving anterior cortex of left tibia.
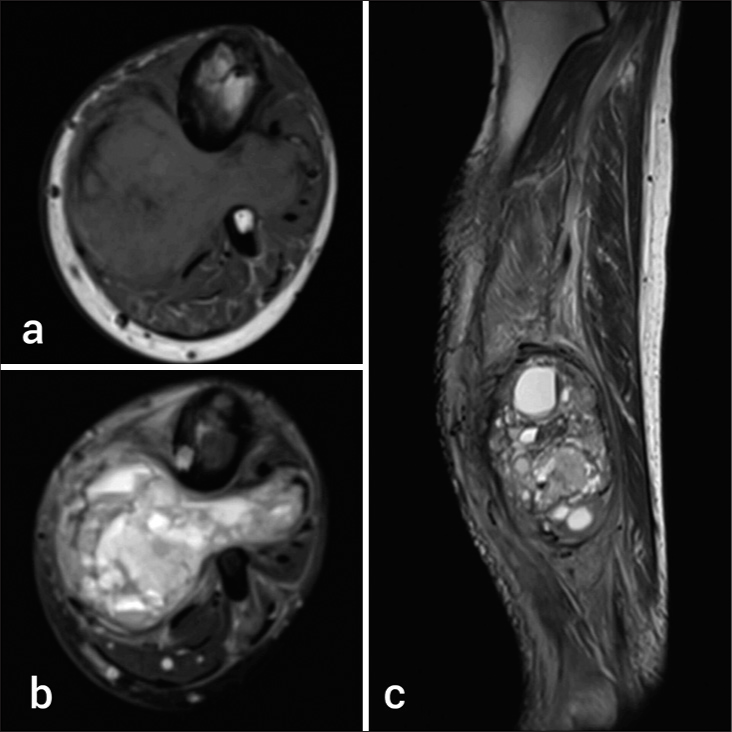
- 40-year-old man with left lower limb swelling. (a) Axial T1-weighted image shows well-defined hypoisointense lobulated dumbbell like mass. (b) Axial T2/Fat saturation and (c) sagittal T2-weighted image showing heterogeneous solid mass with multiple cystic spaces showing fluid-fluid levels within. There is reactive cortical thickening and scalloping over contiguous shafts of tibia and fibula.
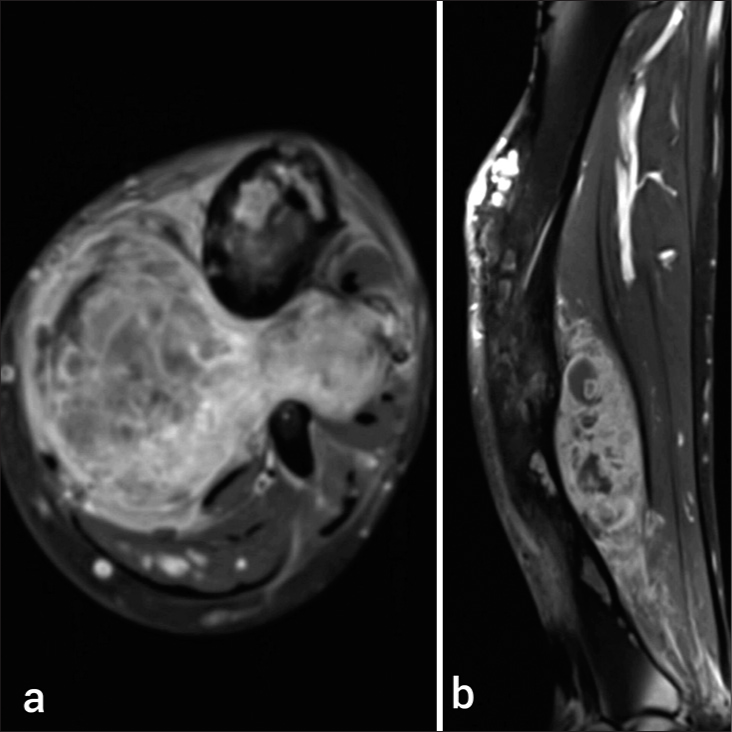
- (a) Axial and (b) sagittal T1 post-contrast images showing heterogeneous contrast enhancement of the lesion. The secondary bone changes are limited to cortex and marrow is free from the disease infiltration.
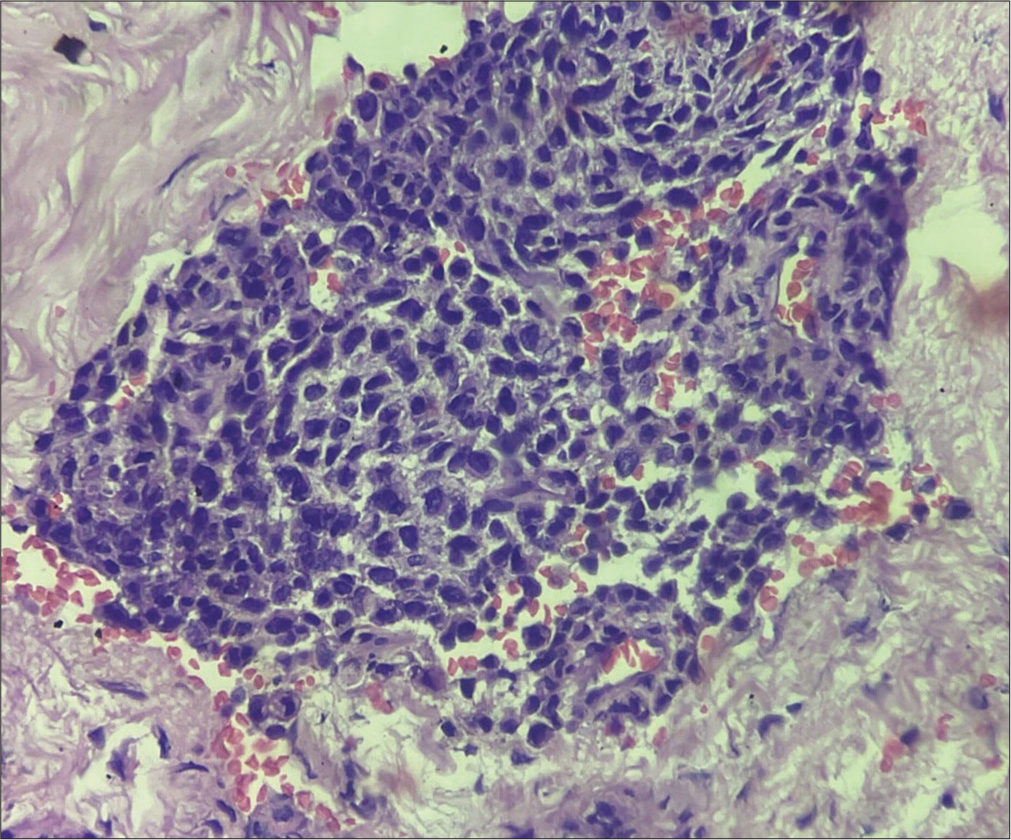
- Nest of ovoid to plasmacytoid cells having monomorphic round nuclei, inconspicuous nucleoli, and clear cytoplasm (×40, hematoxylin and eosin stain).
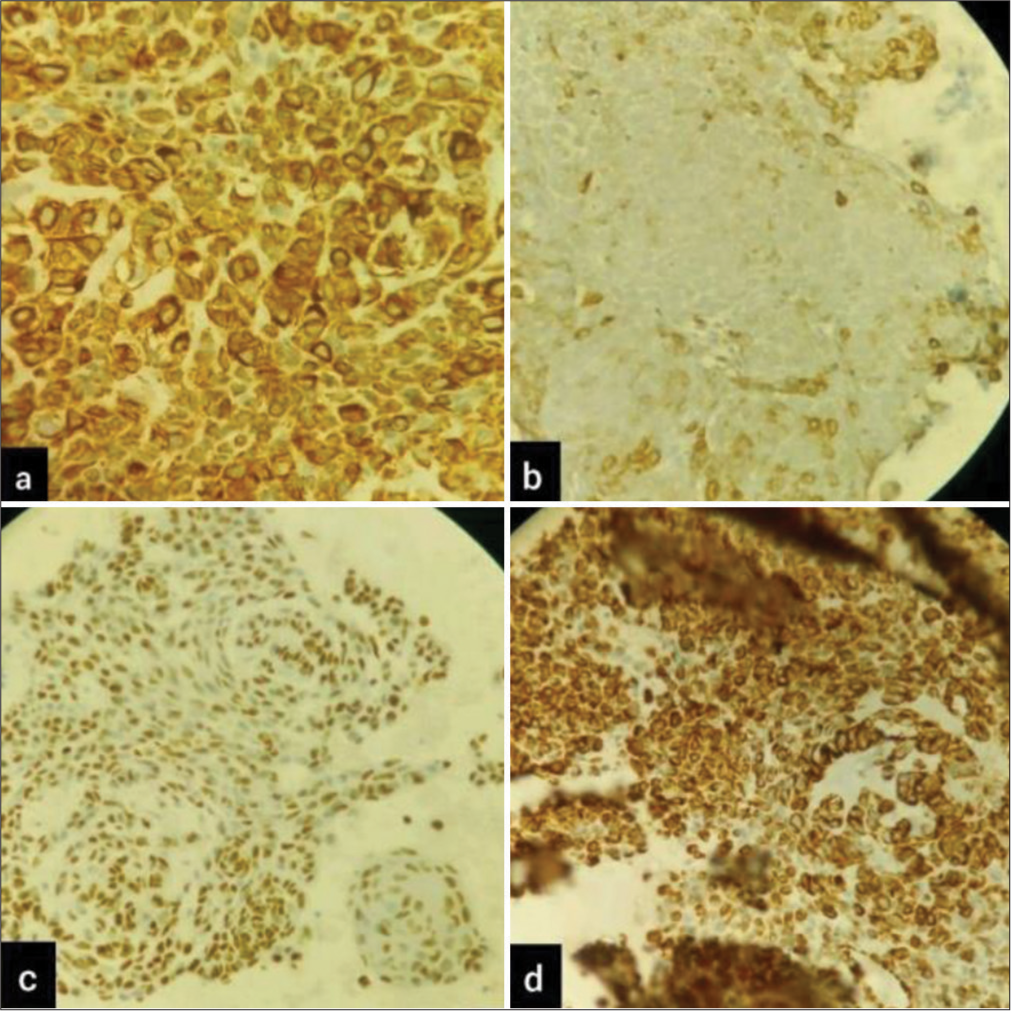
- Immunohistochemistry slides postive for (a) AE-1 (b) p40 (c) CK5/6 (d) vimentin markers.
DISCUSSION
Soft-tissue myoepithelial tumors are uncommon, but they have been observed more frequently in the past decade. Soft-tissue myoepithelial carcinomas are equally prevalent in both genders, and lesions most frequently arise in the extremities and limb girdles.
Like their counterparts in the salivary glands,[3,4] myoepithelial tumors of soft tissue exhibit a variety of morphologic and immunophenotypic characteristics. Tumors are categorized as mixed tumor/chondroid syringoma, myoepithelioma, and myoepithelial carcinoma; in soft tissue, tumors with at least moderate cytologic atypia are considered malignant. Myoepithelioma mainly consists of spindled or ovoid myoepithelial cells, characterized by nuclei with minimal or no atypia, fine chromatin, and small to inconspicuous nucleoli. Myoepithelial carcinomas are characterized by moderate-to-severe atypia, with vesicular nuclei and prominent nucleoli; cytologic atypia has been identified as the only predictor of aggressive behavior in soft-tissue tumors.[3,5] Although high mitotic rates and necrosis are frequently observed in myoepithelial carcinoma, they do not consistently predict aggressive behavior.[3,5] As a result, myoepithelial carcinomas are graded as low, intermediate, or high based on the extent of cytologic atypia, along with the presence of mitoses and necrosis.
There are multiple case reports describing histologically proven cases of myoepithelial soft-tissue tumors in various anatomical locations from head to toe. Imaging findings are often nonspecific and overlap with multiple commoner entities such as soft-tissue sarcomas and metastasis. Therefore, this tumor is infrequently described in radiology literature, with only a few dedicated radiology case reports. In a study of 22 patients of myoepithelial cell carcinoma of bone and soft tissue by Aiba et al.,[6] the tumors of bony origin showed geographic or moth-eaten (permeative) radiographic appearance classified as type II and IIIB of modified Lodwick-Madewell classification. Among the tumors of soft-tissue origin, the most common growth pattern was a focally invasive, followed by diffusely invasive and well-defined lesions. The lesion in our case also showed focally invasive pattern with muscular and neurovascular invasion. Initial evaluation with ultrasound can be useful in cases of soft-tissue tumors where radiographic appearance is just suggestive of soft-tissue fullness. Vascular invasion, thrombosis, and heterogeneous appearance of the lesion, with vascularity and internal necrosis or fluid levels can be helpful in differentiating locally aggressive myoepithelial tumors from benign soft-tissue tumors such as hemangiomas, fibromas, and lipomatous tumors. However, radiological appearances are less likely to provide adequate differentiation between malignant soft-tissue tumors, where histopathology with IHC is confirmatory.
The primary treatment for localized soft-tissue myoepithelial carcinoma is surgical resection with clear margins after which adjuvant therapy is considered. However, due to rare occurrence, there is no standard treatment which is available. Pre- or post-operative radiation can be useful. However, even with optimal treatment, 40–45% of patients experience metastatic or recurrent disease.[2,5] Positron emission tomography-computed tomography is useful for monitoring metastatic or recurrent tumors and distinguishing them from any co-exiting benign pathologies or post-treatment effects. Monotherapy or combine chemotherapy may help in managing advanced cases, with drugs such as doxorubicin, carboplatin, cyclophosphamide, and vinorelbine being explored as palliative options. Although systemic therapy may show some effectiveness, more robust treatments are needed, and participation in clinical trials is encouraged.[3]
Our case report is unique in describing florid secondary bone changes due to chronic remodeling in bones as a result of mass effect of the tumor. Bowing deformity of tibia with disorganized new bone formation along convex margins is probably secondary to stress induced microfractures along the convex surface. Such bony changes can mimic bony lesions like sabre tibia deformity of Paget’s disease or osteofibrous dysplasia. MRI can be useful in differentiating secondary bone changes from other neoplastic etiologies, as it can help in tissue characterization and assessing secondary marrow involvement. Unfortunately, our patient did not undergo a bone biopsy for the confirmation of secondary bone changes.
To the best of our knowledge, there is no case report of myoepithelial tumor showing fluid-fluid levels within. Fluid-fluid levels have been reported in multiple soft tissue tumors like hemangiomas, schwannomas, leiomyosarcoma, liposarcoma, malignant fibrous histiocytoma, myxofibrosarcoma, primitive neuroectodermal tumors, and a variety of sarcomas.[7] It is a non-specific imaging finding and cannot reliably differentiate benign versus malignant nature of tumor. However, in the evolving course of radiological knowledge of myoepithelial tumors, this case report can provide a valuable insight into its imaging appearance.
CONCLUSION
Myoepithelial tumors in soft tissue are uncommon tumors with radiological and pathological heterogeneity. They are an important differential consideration for soft-tissue tumors due to their relatively less aggressive nature and better outcomes compared to more aggressive tumors such as sarcomas and metastases. Coexisting bony changes in adjacent bones surrounding the tumor should be evaluated with caution for secondary bony remodeling versus tumor infiltration or coexisting bone lesions. Combination of radiographs and MRI can provide valuable information pertaining to primary soft-tissue tumor and its remodeling effects on the adjacent bones.
Lack of infiltration into adjacent muscles, bones, and microvasculature, along with long-standing history and secondary bone changes of chronic remodeling, are soft pointers toward less aggressive nature of the tumor; however, histopathology is confirmatory. When diagnosing certain conditions, a multidisciplinary approach works well. We can diagnose such rare diseases via a multidisciplinary approach for better management of patients and to improve clinical outcomes.
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Myoepithelial tumor of soft tissue: Histology and genetics of an evolving entity. Adv Anat Pathol. 2014;21:411-9.
- [CrossRef] [PubMed] [Google Scholar]
- Myoepithelial neoplasms of soft tissue: An updated review of the clinicopathologic, immunophenotypic, and genetic features. Head Neck Pathol. 2015;9:32-8.
- [CrossRef] [PubMed] [Google Scholar]
- Adult soft tissue myoepithelial carcinoma: Treatment outcomes and efficacy of chemotherapy. Med Oncol. 2020;37:13.
- [CrossRef] [PubMed] [Google Scholar]
- Myoepithelial carcinoma of the salivary glands: A clinicopathologic study of 25 patients. Am J Surg Pathol. 2000;24:761-74.
- [CrossRef] [PubMed] [Google Scholar]
- Myoepithelial tumors of soft tissue: A clinicopathologic and immunohistochemical study of 101 cases with evaluation of prognostic parameters. Am J Surg Pathol. 2003;27:1183-96.
- [CrossRef] [PubMed] [Google Scholar]
- Histological and imaging features of myoepithelial carcinoma of the bone and soft tissue. Skeletal Radiol. 2024;53:2617-25.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence and diagnostic significance of fluid-fluid levels in soft-tissue neoplasms. Clin Radiol. 2007;62:769-74. discussion 775
- [CrossRef] [PubMed] [Google Scholar]




